Article Text

Abstract
Despite mass population screening and an incidence of EGC in Japan that is at least double that of the West, there seem to be no genuine differences in the clinicopathological features of the disease between the two regions. The macroscopic appearance, size, depth of invasion, frequency of lymph node invasion, and histology of EGC are all remarkably similar in Japan, Europe and America, as are sex and age distributions.
Patients with EGC are a number of years younger than those with advanced cancer. This is not surprising: Tsukuma et alfollowed 56 cases of EGC that were not surgically treated and estimated that the median “duration of EGC” before becoming advanced was 37 months.87 This suggests that EGC undergoes a period of slow growth before becoming advanced. Further differences between early and advanced cancers include a higher frequency of synchronous cancers and a longer symptom duration in EGC.
Unfavourable prognostic factors in EGC include lymph node invasion, and invasion through the muscularis mucosae, though it is not clear whether these are independent. Repeated attempts have been made to identify other prognostic factors, but no clear pattern has emerged, with the possible exceptions of patient age, tumour size, and the presence of ulceration.
The postsurgical outcome of EGC in the West is marginally less favourable than in Japan. In view of the similar clinical and pathological features in the two regions it seems likely, therefore, that this is because of the more aggressive surgical techniques traditionally used in Japan. Conversely, however, EMR has recently emerged as an important technique in Japan. Despite the advantages of low operative mortality and normal function of the postoperative stomach, there are also a number of potential disadvantages. It would seem sensible, therefore, to await the results of long term follow up studies before widespread adoption of EMR in Europe. Nevertheless, this technique should be considered for frail patients unfit for more radical surgery.
Statistics from Altmetric.com
Early gastric cancer (EGC) was first defined in 1962 by the Japanese Society of Gastroenterological Endoscopy as adenocarcinoma confined to the mucosa or submucosa irrespective of lymph node involvement.1 The need for such a definition was based on the observation that gastric cancer of this type had a favourable prognosis. Indeed, this had been recognised as early as 1938 by Saeki who reported that patients who had gastric cancer confined to the submucosa had a five year survival in excess of 90%.2
Since this classification was devised there has been enormous interest in EGC. Five year survival rates of greater than 90% have repeatedly been reported in Japan, and more recently, in some centres in the West. As a consequence, screening of the asymptomatic population for EGC has been implemented in Japan, Chile3and Venezuela.4 In Europe, and elsewhere, screening has targeted high risk groups, while others have advocated a low threshold for the investigation of dyspepsia. Despite enormous costs, little prospective evidence exists for the ability of such programmes to reduce mortality from gastric cancer.
It continues to be debated, however, whether gastric cancer, and in particular EGC, behaves differently in Japan and the West. This is because Japanese surgeons have, at least until recently, reported better survival rates than their Western counterparts. A variety of reasons for this discrepancy has been offered, including differences in operative technique, population characteristics, and the natural history of the disease.
In this paper we review the European and Western experience of EGC and compare this with the Japanese. A Medline literature search looking for articles on EGC from 1971 to 1996 was performed. All such papers were scrutinised for additional relevant references. Data were tabulated and, whenever possible, this is depicted graphically. In some cases, figures were calculated from data quoted in the text. Clinical features, histopathology, prognostic factors, and survival rates of EGC are all examined, as well as differences between EGC and advanced gastric cancer (AGC).
In total, 72 EGC case series were reviewed. From Europe, there were 30 papers, 10 of which were from Italy. The remainder were from the UK (eight papers), Germany (three), Netherlands (two), Portugal (two), Switzerland, Sweden, Austria, Spain, and France (one each).5-34 Further papers were also reviewed from the USA (six), Canada, Brazil, and Australia (one each).35-43From Japan there was a total of 32 papers,44-75 and from Korea there was one.76 The number of patients in each case series was highly variable. In the European literature it ranged from 11 patients to 271,15 ,30 whereas in Japan numbers were much higher, up to 17 212.47 These differences reflect both the higher incidence of gastric cancer in Japan and the determined efforts of the Japanese to combat this disease over the past three decades, resulting in large centres of excellence dedicated to the management of cancer.
Incidence of EGC
The majority of Western series report the incidence of EGC to be 10–20% of resected cancers. When all cases (including palliative surgery and patients unsuitable for surgery) are considered, the incidence falls to around 10%. This, however, is probably an overestimation of the incidence in the community, as these data are almost universally taken from surgical cohorts. When pathological records are examined, the incidence falls further: Ballantyne et al, for instance, report an incidence of EGC in 3.9% of pathological specimens in the Nottingham General and University Hospitals between 1978 and 1985.18 Even this, however, does not take into account cases first reported on death certificates. None the less, the incidence of EGC is increasing in many centres in Europe, reflecting the increased use of gastroscopy,19although not yet approaching the high levels found in Japan.
The Japanese national records show that the percentage of early cancers among resected cases was 40% in 1985 with a gradual increase in detection rates throughout the country over the preceding 20 years,57 whereas in the Cancer Institute of Tokyo the percentage of EGC overtook advanced cancers in 1990.58Again, this is probably an overestimation of the true incidence of EGC in the community. It is none the less clear that EGC is detected considerably more frequently in Japan than in Europe. The reason for this discrepancy is almost certainly the mass screening of the asymptomatic population introduced in 1957, though, as in Europe, the upward trend is closely paralleled by advances in diagnostic technology.
Histopathology
MACROSCOPIC APPEARANCE
The most widely used classification of EGC is based upon the macroscopic appearance of the tumour (fig 1). EGC is divided into tumours that are protruded (I), superficial (II), and excavated (III).1 Type II is further subdivided into elevated (IIa), flat (IIb), and depressed (IIc). Generally, the elevation of type IIa is less than twice the thickness of the adjacent mucosa, whereas in type IIb no elevation or depression can be seen, and in type IIc the depression is only erosion.51 Combinations of the five lesions are common, (for instance, a shallow depression (IIc) with a central excavation (III) is classified as type IIc + III).

: Macroscopic classification of early gastric cancer according to the Japanese Research Society for gastric cancer.
On the whole, the majority of EGC contain a depressed or ulcerated component with types IIc or III, or both, pre- sent in greater than 60% (fig 2). This is true for both Western and Japanese series. The remainder are mainly elevated, with only a very small number of flat lesions (type IIb) being identified. This no doubt reflects not only the fact that ulcerated lesions are easier to detect, but also that a large number of EGC ulcerate as part of their natural history, an observation first made by Sakita et al, who proposed the “life cycle of the malignant ulcer”77 in which there is ulceration and healing, followed by re-ulceration. When flat lesions are detected, however, they are characterised simply by a reddening or pallor of the mucosa. They are usually of minute or small size, and limited to mucosal invasion, suggesting that they are at an early stage in their natural history.70 ,71

: Macroscopic classification of early gastric cancer: per cent of lesions that are depressed or excavated, or a combination of the two (IIc, III, IIc + III).
SIZE
The size of EGC varies greatly, ranging from less than 0.5 cm to 7.0 cm.6 Mean size is reported between 1.7 cm and 3.0 cm in Europe and the USA.6 ,35 ,36 With advancing diagnostic techniques, the proportion of smaller sized lesions is increasing. This is especially true in Japan.44 ,47 ,48 ,58 ,78 Xuan et al reviewed 2846 cases of EGC in Japan, and found the frequency of lesions less than 3 cm increased from 28 to 56% between 1962 and 1987.48
Lesions with a maximum diameter of 5 mm or less are classified as minute, and those with a diameter of between 6 and 10 mm as small. These lesions tend to be flat (type IIb) and histologically well differentiated.70 Fukutomi and Sakita report that minute lesions accounted for 2.9% of EGC in 1972 and 4.2% in 1980, and small lesions for 6.8% in 1972 and 10.1% in 1980.47 However, in a recent report from Italy, minute lesions accounted for 12% and small lesions for 23% of EGC,5 whereas Chia et al (Australia) report 21% small or minute lesions.43 Thus, it would seem that there is no great difference in the size of lesions detected on separate continents.
MICROSCOPIC APPEARANCE
Depth of invasion
The definition of EGC allows for invasion only as far as the submucosa, without penetration through the muscularis propria. However, EGC can be divided into those that invade the mucosa only, and those that penetrate the muscularis mucosa to the submucosa. Figure 3 shows the proportion of each type. Although there is wider variation between the smaller Western series, the division is generally around 50% for both mucosal and submucosal invasion in both Japan and Europe.

: Early gastric cancer and depth of invasion: per cent of lesions that have invaded mucosa alone or have invaded into the submucosa.
Depth of invasion may be predicted by macroscopic type, with polypoid and ulcerated/eroded lesions having deeper invasion than flat lesions. Fukutomi and Sakita reported 17 212 cases of EGC from Japan; the ratio of mucosal to submucosal invasion was 6.9 and 2.1, respectively, for types IIb and IIa, compared with a ratio of 1.03, 0.97 and 0.45 for types I, III and IIa + IIc, respectively.47
Histological diagnosis
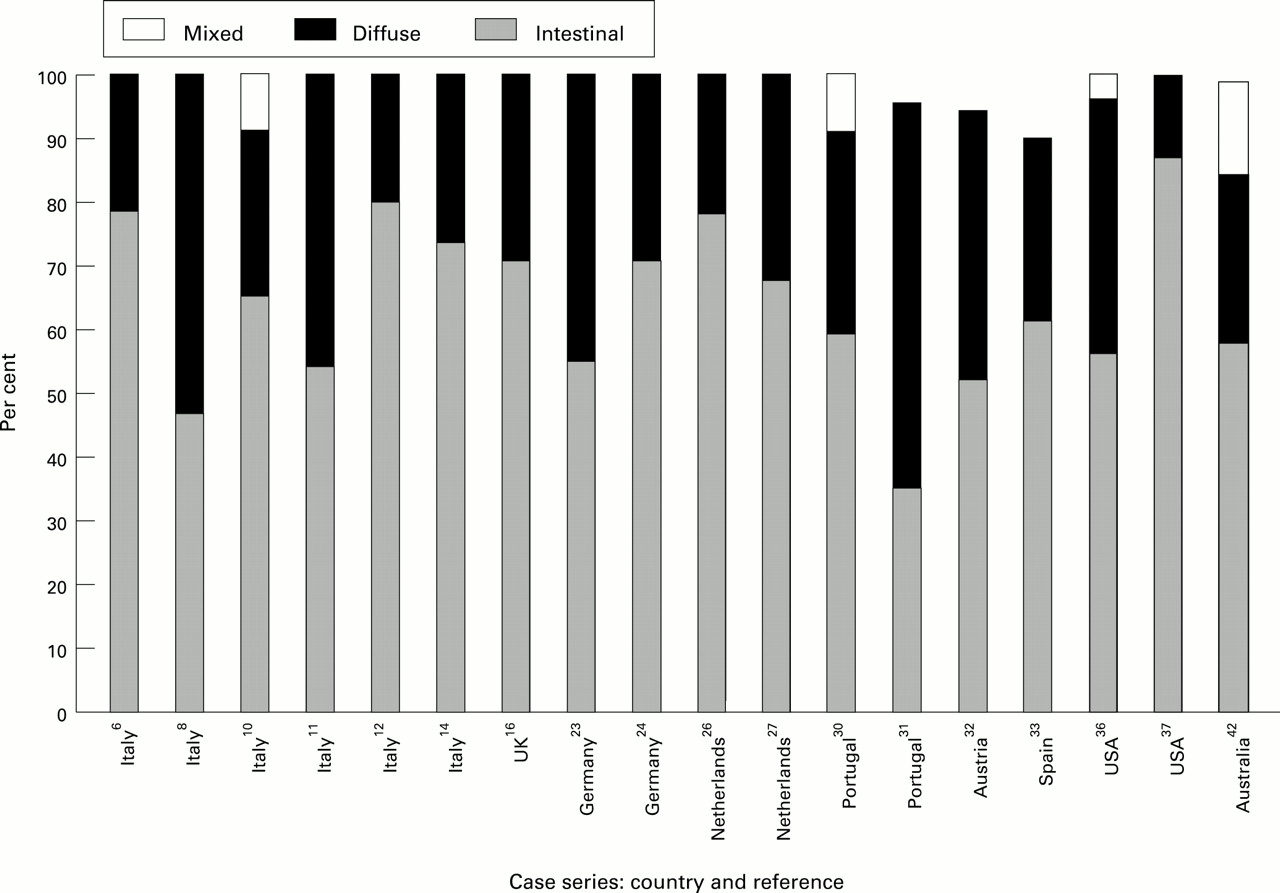
A helpful pathological classification for gastric cancer was described by Lauren in 1965.79 Tumours are divided into those with gland formation (intestinal type) and those without glandular characteristics (diffuse type). Intestinal type occurs more commonly in older patients in areas with a high incidence of gastric cancer, whereas diffuse type has a constant rate worldwide and occurs in a younger age group. This classification is in widespread use in the West. In EGC intestinal type predominates, accounting for more than half of the patients in 16 of 18 reports, and more than 70% in seven of the 18 (fig 4).

: Early gastric cancer according to the Lauren classification: per cent of cases with intestinal, diffuse, or mixed histology.
Comparison with the Japanese experience is difficult as the Lauren classification is not frequently quoted. Instead, tumours are classified according to the Japanese Research Society Committee80 and are divided into papillary, tubular/well differentiated, and tubular/moderately differentiated adenocarcinoma (which together are considered well differentiated, and correspond to intestinal type), poorly differentiated and signet ring adenocarcinoma (which together correspond to poorly differentiated or diffuse cancer), and mucinous adenocarcinoma. Taken together, differentiated tumours account for around 60% and undifferentiated for 40% (table1).44 ,48 ,50 ,53 ,55 ,56 This compares closely with the Western experience.
Histological classification of early gastric cancer in the Japanese literature
It has been reported that the degree of differentiation is closely related to depth of invasion for gastric cancer, with poorer differentiation evident in submucosal and advanced cancers than mucosal lesions.10 ,41 ,50 This requires confirmation (indeed Eckardt et al report very similar degrees of differentiation between EGC and AGC23), but suggests that either poorly differentiated tumours are more aggressive, or that tumours undergo transformation to a less differentiated type as growth progresses.
It is also worthy of note that there may be some discrepancy in the reporting of degree of differentiation, and even between the classification of benign and malignant disease. Fujii et al reported 30 cases of EGC from Japan defined as tub 0, that is, very well differentiated tubular adenocarcinoma.54These tumours demonstrated reduced size, invasion and lymph node metastasis compared with other less well differentiated tumours, and were described as “less malignant”. They were only identified on the basis of cellular atypism and it is possible that other authors may have classified these tumours as benign. This potential discrepancy in classification is important to recognise when comparing incidence and survival rates between countries.
LYMPH NODE INVASION
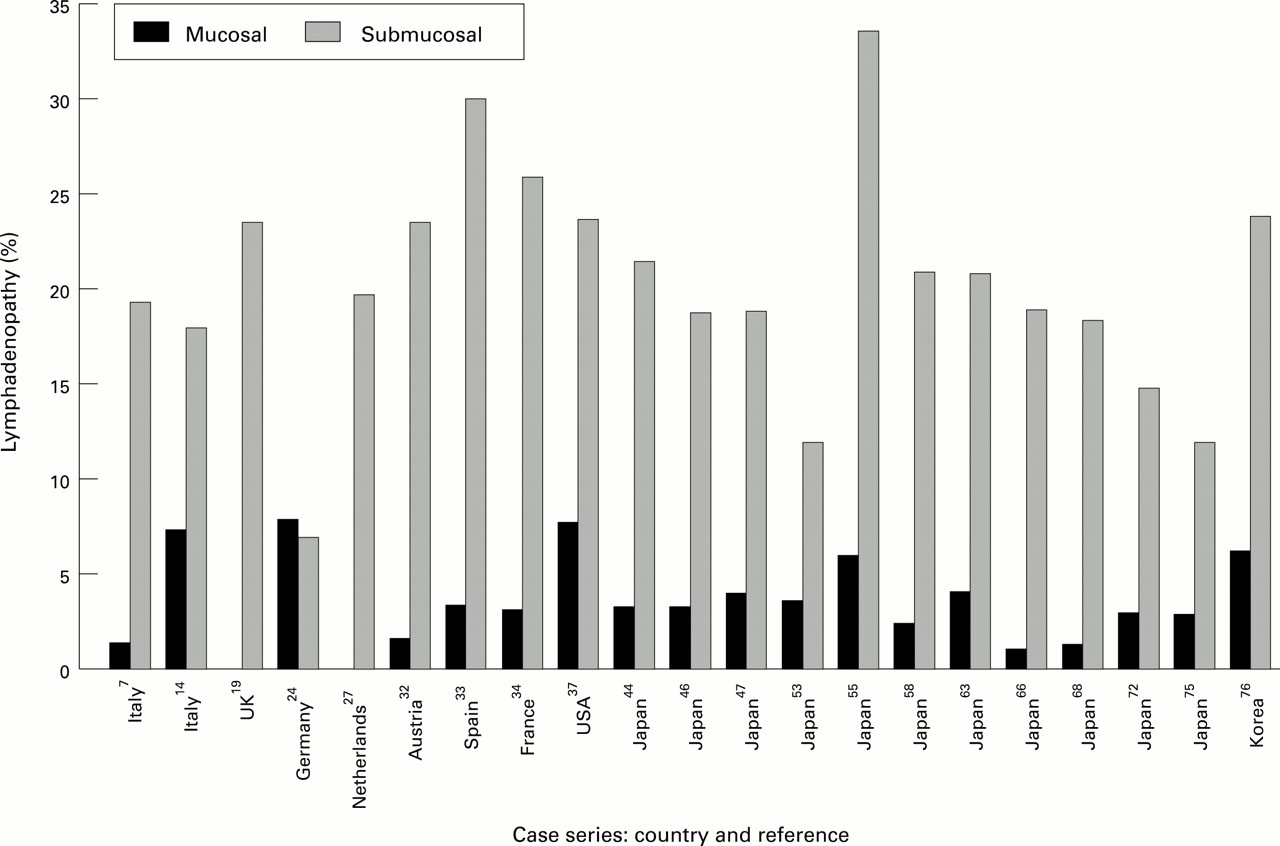
Despite only minor local invasion in EGC (by definition) lymph node invasion is still relatively common, with rates varying between 10 and 20% in most reports (fig 5). The presence of nodal metastases is very closely related to depth of local invasion (fig 6). With submucosal invasion, lymph nodes are involved in between 15 and 30%, but with mucosal lesions, lymph node involvement is much less common (0–7%). Furthermore, lymph node invasion is commoner with larger tumours,5 ,34 ,46 ,49 ,53 ,76 and possibly with poorly differentiated tumours,34 although this relation is reported less consistently.

: Lymphadenopathy in early gastric cancer: per cent of cases with involved lymph nodes detected at time of operation.

: Lymphadenopathy in early gastric cancer according to depth of invasion: per cent of cases with involved lymph nodes detected at time of operation, divided into cases of mucosal invasion alone and cases in which the submucosa has been invaded.
In all but one series,9 where lymph node staging is reported the majority (more than 70%) of lymph nodes involved are N1. The rest are usually N2, but on a few occasions more distant involvement of N3, and rarely N4, nodes has been reported.44 ,45 ,58 This is only seen in the Japanese literature, but is probably owing to the more extensive surgical resection and the meticulous examination of the postoperative specimen.
DISTANT METASTASES
Liver/haematogenous metastases are rare at the time of diagnosis of EGC, and were reported in only two of the case series reviewed.62 ,68 Although this may be biased owing to the reporting of potentially curative surgery alone, it is consistent with the high postoperative survival rates and the benign nature of this disease.
SYNCHRONOUS CANCERS
The concept of multiple synchronous gastric cancers is well recognised. The criteria for diagnosis was first established by Moertelet al in 195781: (a) each lesion must be of pathologically proven malignancy; (b) all lesions must be distinctly separated by intervals of microscopically normal gastric wall; and (c) the possibility that a lesion represents local extension or metastasis must be ruled out beyond any reasonable doubt.
When reported, the prevalence of synchronous cancers is between 2 and 14% in European literature (apart from Gardiner et al who amazingly found 14 of 30 EGC to be multifocal15). This closely echoes the Japanese experience of 5–13%. In addition to double tumours, triple and quadruple tumours have also been reported.34 ,52 ,82 Synchronous EGC, however, do not differ from their solitary counterparts with regard to pathological features.51
It has been found that the frequency of multiple tumours is commoner in EGC than AGC,23 ,82 and this has been taken to imply that progressive carcinoma represents convergence of multiple primary foci. Furthermore, many synchronous tumours are only detected at the time of operation. Noguchi et al reported successful preoperative diagnosis of synchronous microcarcinoma in only 35% of those cases in which they were eventually demonstrated after resection.51This implies that even careful endoscopic examination of the stomach misses large numbers of small EGC, an important point when the efficacy of screening is considered.
It has been suggested that patients with EGC are predisposed to developing cancer at other sites. Although this may be true for patients with cancer as a rule, there is no compelling evidence that EGC behaves differently from other tumours in this respect. Notwithstanding this, the presence of multiple synchronous tumours suggests that EGC represents a field change of the gastric mucosa as a whole, indicating a high risk of developing further tumours in the rest of the stomach.
Clinical features
AGE AND SEX DISTRIBUTION
As in AGC, there is a strong male predominance in EGC. In the European literature the male:female ratio varies from 1 to 4.75.15 ,26 Sex ratio was stated in 24 European case reports: of 1730 cases in these reports, there was a mean male:female ratio of 1.66. In the Japanese literature, the male:female ratio was reported in five series, totalling 21 590 cases, with a mean of 1.97. This is only slightly higher than the European mean, but may reflect higher screening rates of the working male population in Japan.
The mean age of patients with EGC was stated in 17 European reports, totalling 1147 cases. Taken together, this gives a mean age of 59.9 years. This is only marginally older than the mean age in Japan (57.8 years; 3378 cases; three case reports); a surprising finding if one considers their screening programme. EGC probably occurs in younger adults than AGC; two series report a difference of eight years,8 ,23 a third of 23 years (though only five cases of EGC),35 whereas a fourth found no difference.6
SYMPTOMS
Owing to the screening of an asymptomatic population, there is little information on the symptoms of EGC in Japan. In Europe the duration of symptoms in EGC is varied but often long. Usually symptoms have been present for longer than six months,18 ,27 and often the mean duration of symptoms is longer than a year.16 ,17 ,26 ,43 When compared with AGC, the time scale of symptoms in EGC is considerably longer.6 ,35 In addition, it has been reported that EGC carries a longer prodrome of symptoms if it is ulcerated, rather than protuberant.16
The presenting symptoms of EGC resemble those of benign gastric ulcer.23 Epigastric pain and dyspepsia are very frequently present (between 60 and 90%). Anaemia is uncommon at presentation, and history of gastrointestinal bleeding is usually present in less than 25%. Weight loss almost always occurs in less than 40% of patients (table 2).6 ,9 ,19 ,23 ,27 ,34 ,36 ,37 In contrast, weight loss is a common, prominent feature of AGC, occurring in about 60% of patients.83
Symptom distribution in early gastric cancer (per cent of patients with specified symptom)
It is difficult to interpret the observation that the EGC symptom profile and duration more closely resemble benign gastric ulceration than advanced cancer. It may suggest either that EGC can exist undetected in the stomach, causing mild symptoms only for long periods of time, or that there is a gradual malignant conversion of benign disease over such a period. Nevertheless, this similarity in clinical features, taken with the notion that these ulcers can undergo a healing phase,77 strengthens the need for aggressive, early investigation of older patients with ulcer-like symptoms.
Treatment of EGC
In general, the most widely and successfully performed operation for EGC is gastrectomy (distal, proximal or total) with radical R2 lymphadenectomy. This is universal in Japan, but has gained increasing acceptance in Europe in recent years.19 Operative mortality is low in Japan, generally less than 1%, compared with a more variable picture in Europe (between 1 and 6.5%19 ,34).
Ironically, although European surgeons have gradually been adopting the more aggressive Japanese methods, the Japanese have simultaneously been concentrating on more conservative surgery. Endoscopic mucosal resection (EMR) was introduced in 1978. It is a relatively simple technique that permits en bloc removal of the tumour. In Japan it is now considered for use in patients with (i) differentiated, elevated type less than 2.0 cm in diameter, (ii) differentiated, depressed type without ulceration, less than 1.0 cm in diameter, and (iii) the undifferentiated, depressed type without ulcer formation, 0.5 cm in diameter.58
At the Cancer Institute of Tokyo58 the use of EMR has been increasing slowly: between 1988 and 1990 it was performed in 23.6% of all early cancers, with a five year survival of 86%. There are theoretical risks, however, in this approach. Firstly, EGC is frequently associated with synchronous tumours that are not detected during endoscopic examination, and would therefore not be removed at the time of EMR. Secondly, even if there are no synchronous cancers, the remaining stomach is likely to contain areas of premalignant change, such as intestinal metaplasia or dysplasia, that would confer a high risk of carcinoma in the future. Thirdly, it is difficult to be sure of the depth of invasion preoperatively, even with endoscopic ultrasound,84 making it extremely difficult to exclude confidently node metastasis preoperatively.
Survival and prognosis
SURVIVAL
The prognosis for early gastric cancer is universally excellent. Almost all Western and Japanese authors are now reporting five year survival rates of over 90% for EGC if relative survival or deaths from gastric carcinoma alone are considered. A small number of series has reported survival rates at 10, 15, and 20 years. The Japanese have demonstrated high relative survival to 10 and 15 years, comparable with the rest of the population.60 ,85 However, if deaths from other causes are excluded, then the survival is lower after 10 years in Western reports, falling to between 84 and 92%.11 ,12 ,17 ,36 In one long term French follow up study, the 15 and 20 year survival rates fell to 58% and 51%, respectively. This included all cause mortality, though, and is consequently difficult to interpret.34
Looking at the recurrence rate of EGC after surgery, the Japanese consistently report a rate of less than 5%. Rates are generally higher in Western reports, usually between 5 and 15%, with rates of less than 5% only being found in a handful of cases (fig7).6 ,12 ,19 ,26 ,33 ,38 While different recurrence rates should be compared with caution, as they are dependent on length of follow up, if they are taken in conjunction with the survival rates it becomes apparent that EGC carries a marginally poorer prognosis in the Western population.

: Recurrence rate of early gastric cancer. The recurrence rate was calculated from data published in the relevant references. It includes patients with recurrence of early gastric cancer regardless of ultimate survival. Operative mortality is excluded. Numbers above columns represent follow up in years (mean or median, as reported in the publication).
PROGNOSTIC FACTORS
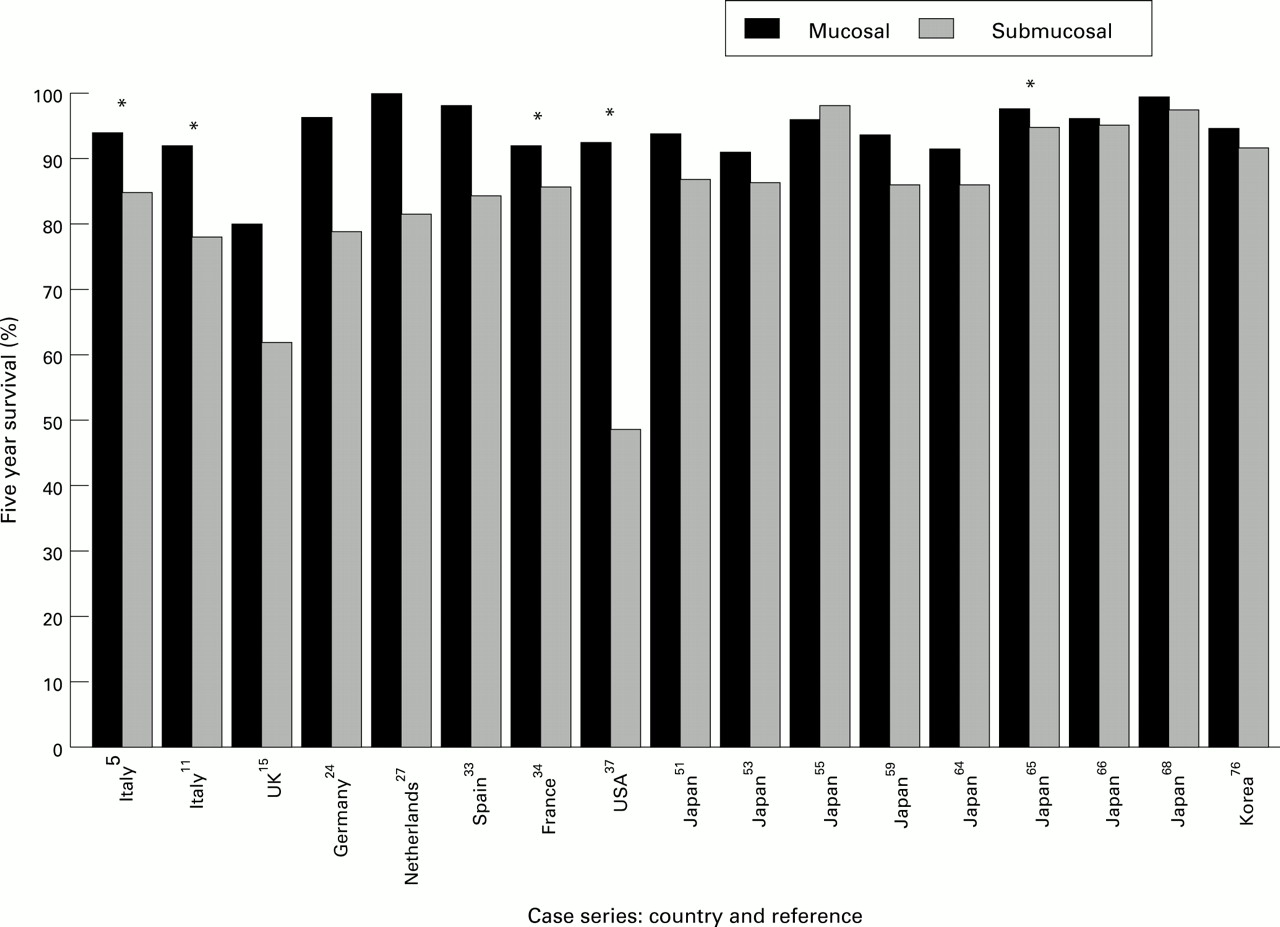
Figure 8 shows the five year survival of early gastric cancer, divided into those with nodal metastasis and those without. It is not surprising that patients who are free of nodal metastases fare better than those with lymphadenopathy. Furthermore, the prognosis of carcinomas confined to the mucosa is consistently better than those that invade the submucosa (fig 9). This survival advantage is maintained to at least 10 years.11 ,34 ,49 ,53 ,55 ,64 ,65It seems possible, however, that depth of invasion is not an independent prognostic factor but merely acts as a marker for those patients at higher risk of lymph node invasion.

: Five year survival of patients with early gastric cancer: prognosis according to presence or absence of lymphadenopathy at time of operation. *Ten year survival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
: Five year survival of patients with early gastric cancer: prognosis to depth of invasion (mucosal or submucosal) at time of operation. *p < 0.05.
Information on other prognostic factors is more variable. Degree of differentiation has been found to either have no prognostic influence12 ,33 ,34 ,37 ,69 or, where a difference is detected, the differentiated/intestinal types have shown worse prognosis.10 ,11 ,24 ,27 ,36 ,50 ,56 ,61 ,62 ,64 ,67 ,68Although this is a consistent finding, it contradicts the observation that less differentiated tumours are associated with deeper invasion and lymph node invasion. Old age seems to confer worse prognosis,11 ,36 ,50 even after multivariate analysis.67 Larger tumour size has been associated with either no difference5 ,34 or with worse survival rates,37 ,65 and excavated/depressed tumours have been associated with a better prognosis.24 ,33 ,39 ,56 ,67