Article Text

Abstract
This is a collaboration between the British Society of Gastroenterology (BSG) and the European Society of Gastrointestinal Endoscopy (ESGE), and is a scheduled update of their 2016 guideline on endoscopy in patients on antiplatelet or anticoagulant therapy. The guideline development committee included representatives from the British Society of Haematology, the British Cardiovascular Intervention Society, and two patient representatives from the charities Anticoagulation UK and Thrombosis UK, as well as gastroenterologists. The process conformed to AGREE II principles and the quality of evidence and strength of recommendations were derived using GRADE methodology. Prior to submission for publication, consultation was made with all member societies of ESGE, including BSG. Evidence-based revisions have been made to the risk categories for endoscopic procedures, and to the categories for risks of thrombosis. In particular a more detailed risk analysis for atrial fibrillation has been employed, and the recommendations for direct oral anticoagulants have been strengthened in light of trial data published since the previous version. A section has been added on the management of patients presenting with acute GI haemorrhage. Important patient considerations are highlighted. Recommendations are based on the risk balance between thrombosis and haemorrhage in given situations.
- endoscopic procedures
This is an open access article published by Thieme and BMJ Publishing Group Ltd under the terms of the Creative Commons Attribution Non Commercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes. (http://creativecommons.org/licenses/by-nc/4.0/)
Statistics from Altmetric.com
Summary of recommendations
Recommendations for the management of patients on antiplatelet therapy or anticoagulants undergoing elective endoscopic procedures are summarised in figures 1 and 2. Risk stratification for endoscopic procedures are detailed in table 1, for antiplatelet agents in table 2, and for heparin bridging in patients on warfarin table 3.
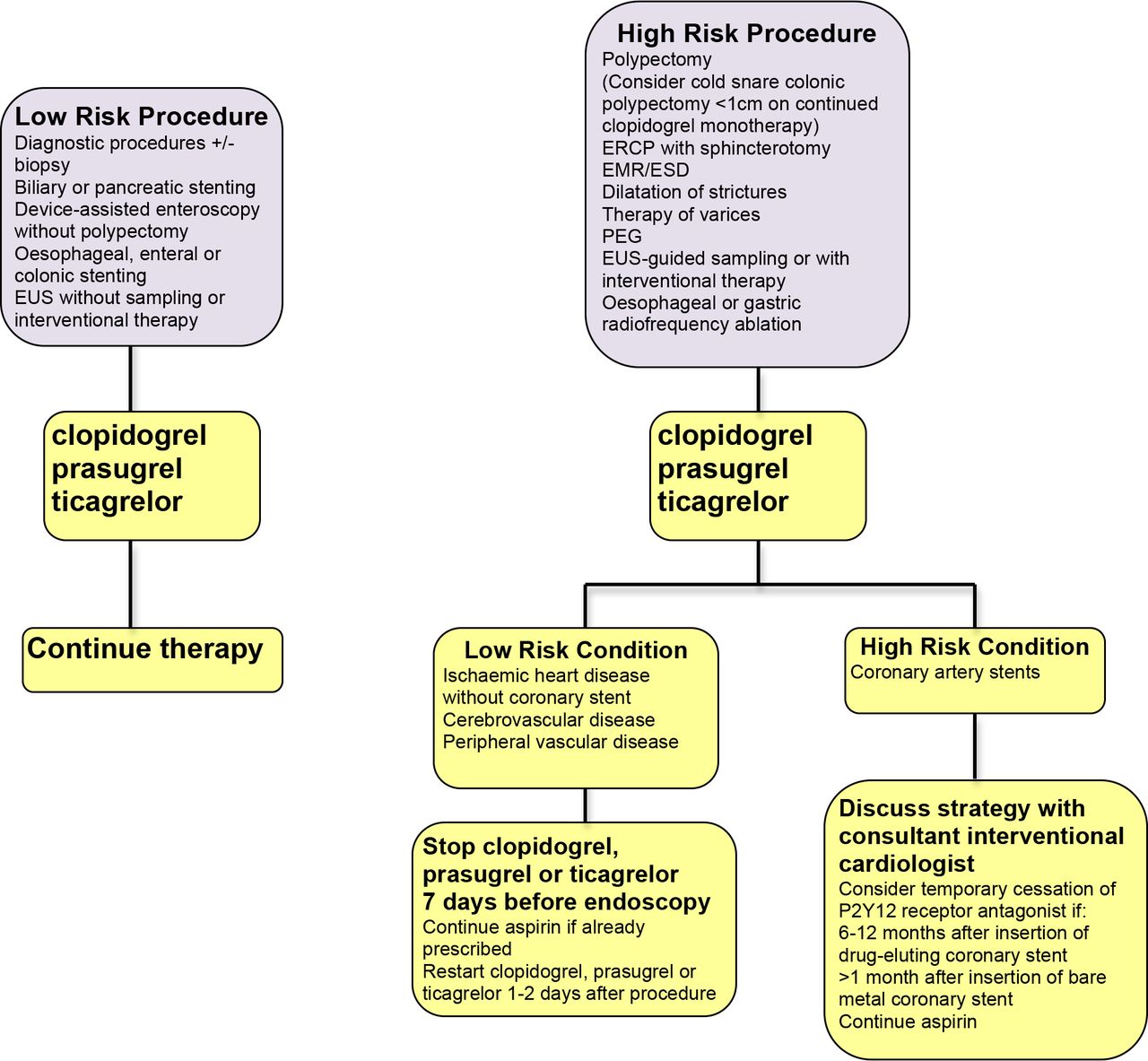
Guidelines for the management of patients on P2Y12 receptor antagonist antiplatelet agents undergoing endoscopic procedures: 2021 update. EMR, endoscopic mucosal resection; ERCP, endoscopic retrograde cholangiopancreatography; ESD, endoscopic submucosal dissection;EUS, endoscopic ultrasound; PEG, percutaneous endoscopic gastroenterostomy.

Guidelines for the management of patients on anticoagulants undergoing endoscopic procedures: 2021 update. *Blood pressure >140/90 mm Hg or on antihypertensive medication. **Previous VTE on anticoagulation and target INR now 3.5.***Depends on haemorrhagic and thrombotic risk, consider extending interval for ESD. AF, atrial fibrillation; EMR, endoscopic mucosal resection; ERCP, endoscopic retrograde cholangiopancreatography; ESD, endoscopic submucosal dissection; EUS, endoscopic ultrasound; INR, international normalised ratio; LMWH, low molecular weight heparin; PEG, percutaneous endoscopic gastroenterostomy; TIA, transient ischaemic attack; VTE, venous thromboembolism.
Risk stratification of endoscopic procedures based on the risks of haemorrhage and of intervention required to treat a complication
Risk stratification for discontinuation of P2Y12 receptor antagonists clopidogrel, prasugrel or ticagrelor based on the risk of thrombosis
Risk stratification for discontinuation of warfarin therapy with respect to the requirement for heparin bridging
We recommend that all patients are advised of the thrombotic risks of discontinuing antiplatelets or anticoagulants, as well as the haemorrhagic risks of continuing therapy (strong recommendation, low quality evidence).
For all endoscopic procedures we recommend continuing aspirin (strong recommendation, low quality evidence), with the exception of ampullectomy (weak recommendation, low quality evidence). If considering aspirin discontinuation, this should be on an individual patient basis depending on the risks of thrombosis versus haemorrhage (weak recommendation, low quality evidence).
Low-risk endoscopic procedures
For low-risk endoscopic procedures we recommend continuing P2Y12 receptor antagonists as single or dual antiplatelet therapy (DAPT) (strong recommendation, low quality evidence).
For low-risk endoscopic procedures we suggest that warfarin therapy should be continued (weak recommendation, low quality evidence). It should be ensured that the international normalised ratio (INR) does not exceed the therapeutic range in the week prior to the procedure (strong recommendation, low quality evidence).
For low-risk endoscopic procedures we suggest omitting the morning dose of direct oral anticoagulants (DOACs) on the day of the procedure (weak recommendation, low quality evidence).
High-risk endoscopic procedures
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing P2Y12 receptor antagonists 7 days before the procedure (strong recommendation, moderate quality evidence). In patients on DAPT, we recommend continuing aspirin (strong recommendation, low quality evidence).
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing warfarin for 5 days before the procedure (strong recommendation, high quality evidence). Check INR prior to the procedure to ensure <1.5 (strong recommendation, low quality evidence).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend continuing aspirin and liaising with a consultant interventional cardiologist about the risk/benefit of discontinuing P2Y12 receptor antagonists (strong recommendation, high quality evidence).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend that warfarin should be temporarily discontinued and substituted with low molecular weight heparin (LMWH) (strong recommendation, low quality evidence).
For high-risk endoscopic procedures in patients on DOACs, we recommend that the last dose of DOACs be taken 3 days before the procedure (strong recommendation, low quality evidence). For patients on dabigatran with a creatinine clearance (CrCl) (or estimated glomerular filtration rate (eGFR)) of 30–50 mL/min we recommend that the last dose be taken 5 days prior to the procedure (strong recommendation, low quality evidence). In any patient with rapidly deteriorating renal function a haematologist should be consulted (strong recommendation, low quality evidence).
Post elective endoscopic procedures
If antiplatelet or anticoagulant therapy is discontinued, then we recommend this should be resumed up to 2–3 days after the procedure depending on the perceived haemorrhagic and thrombotic risks (strong recommendation, moderate quality evidence).
For all patients on antiplatelets or anticoagulants we recommend advising that there is an increased risk of post-procedure haemorrhage compared with patients not on these drugs (strong recommendation, low quality evidence).
Acute GI haemorrhage
We suggest that permanent discontinuation of aspirin for primary prophylaxis should be considered (weak recommendation, low quality evidence).
We suggest that aspirin for secondary prevention should not be routinely stopped. If it is stopped, it should be recommenced as soon as haemostasis is achieved, or there is no further evidence of haemorrhage (strong recommendation, moderate quality evidence).
We recommend that DAPT is continued if possible in patients with coronary stents in situ and management should be in liaison with a consultant interventional cardiologist (strong recommendation, moderate quality evidence). In the case of major haemorrhage we recommend continuing aspirin if the P2Y12 receptor antagonist is interrupted (strong recommendation, moderate quality evidence). P2Y12 receptor antagonist therapy should be re-instated within 5 days, if still indicated (strong recommendation, moderate quality evidence).
We recommend withholding oral anticoagulant and correcting coagulopathy according to the severity of haemorrhage and the patient’s thrombotic risk in coordination with a consultant cardiologist/haematologist. The correction of coagulopathy should not delay endoscopy or radiological intervention (strong recommendation, low quality evidence).
In patients with haemodynamic instability who take vitamin K antagonists (VKAs), we recommend administering intravenous vitamin K and four-factor prothrombin complex concentrate (PCC) (strong recommendation, low quality evidence), or fresh frozen plasma if PCC is not available (weak recommendation, very low quality evidence).
In patients with haemodynamic instability who take DOACs, we suggest considering the use of reversal agents: idarucizumab in dabigatran treated patients, and andexanet in anti-factor-Xa (anti-FXa) treated patients (weak recommendation, low quality evidence), or intravenous four-factor PCC if andexanet is not available (weak recommendation, very low quality evidence).
We recommend restarting anticoagulation following acute GI haemorrhage in patients with an indication for long-term anticoagulation (strong recommendation, low quality evidence). In patients at low thrombotic risk, we suggest restarting anticoagulation as soon as possible after 7 days of anticoagulant interruption (weak recommendation, low quality evidence). In those at high-thrombotic risk, an earlier resumption of anticoagulation with heparin bridging, preferably within 3 days, is recommended (strong recommendation, low quality evidence).
Introduction and methods
The British Society of Gastroenterology (BSG) and the European Society of Gastrointestinal Endoscopy (ESGE) jointly published guidelines on endoscopy in patients on antiplatelet or anticoagulant therapy, including DOACs in 2016.1 2 This is a scheduled 5-year update on the previous guidelines.
These guidelines were drafted by a working party comprising members of the BSG and ESGE, two haematologists representing the Thrombosis and Haemostasis Task Force of the British Society of Haematology, an interventional cardiologist representing the British Cardiovascular Intervention Society (BCIS), and two patient representatives from the charities Anticoagulation UK and Thrombosis UK. Guidelines were prepared according to AGREE II principles3 and comply with the requirements of the National Institute for Health and Care Excellence (NICE). Clinical questions were formulated using the Patients, Interventions, Controls, Outcomes system. Search strategies were delegated to authors with responsibilities for specific sections. Literature searches were conducted using PubMed and OVID Medline, Embase and Cochrane Library. Additional searches were conducted using Google. Literature searches were run up to November 2020, and this time-point should be the starting point in the search for new evidence for future updates to these guidelines. Quality of evidence and strength of recommendations were determined by the authors, and consensus achieved according to the GRADE system.4 After agreement on a final version, the manuscript was subjected to internal peer review and revision by the BSG and the ESGE and sent to all individual ESGE members and member societies prior to publication. Conflict of interest statements were submitted by all authors and are listed at the end of this manuscript. This guideline was issued in 2021 and will be considered for review in 2026, or sooner if new evidence becomes available. This guideline has been co-published with permission in both Gut and Endoscopy.
Patient considerations
We recommend that all patients are advised of the thrombotic risks of discontinuing antiplatelets or anticoagulants, as well as the haemorrhagic risks of continuing therapy (strong recommendation, low quality evidence).
For all patients on antiplatelets or anticoagulants we recommend advising that there is an increased risk of post-procedure haemorrhage compared with patients not on these drugs (strong recommendation, low quality evidence).
As discussed, management of antithrombotic drugs is a balance of the risks of haemorrhage from the procedure versus the risks of thrombosis if antithrombotic medication is discontinued or modified. Haemorrhage secondary to high-risk endoscopic procedures can often be controlled by further endoscopic therapeutic measures, and is rarely fatal. A thrombotic stroke may result in lifelong disability, and a major cardiac event may result in death. Not only do the risks of thrombosis versus haemorrhage need to be assessed on an individual patient basis, but patients should be fully informed, and involved in this decision-making process. The risk of a potentially catastrophic thrombotic event such as a stroke may not be acceptable to a patient even if that risk is very low.
Once the decision to modify antithrombotic medication is made, then a personal plan for that patient should be made. This should include written as well as verbal information regarding the precise timing of any changes. This should include the time of last dose of a drug, and first dose when restarting. If multiple drugs are involved, or substitutions including bridging with heparin, then timing respective to each drug should be clearly communicated. Simple algorithms such as those illustrated in the PAUSE trial for DOACs5 may be useful (figure 3). Late haemorrhagic complications may occur one to 2 weeks after endoscopic therapy, and antithrombotic therapy will have often been reinstituted prior to this. Patients on antithrombotics should be advised that there is a possible increase in postprocedure haemorrhage, and also advised how to seek urgent medical advice at any time of the day or night. We have produced a patient information sheet based on this guideline to assist with patient engagement (online supplemental file).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Perioperative direct oral anticoagulant (DOAC) management protocol. Reproduced with permission from Douketis et al.5 Copyright (2019) American Medical Association. All rights reserved. No DOAC was taken on certain days (shaded) and on the day of the elective surgery or procedure (including endoscopy). The light blue arrows refer to an exception to the basic management, a subgroup of patients taking dabigatran with a creatinine clearance (CrCl) less than 50 ng/mL. The orange arrows refer to patients having a high-bleed-risk procedure. Dark blue arrows refer to patients having a low-bleed-risk procedure. The thickened orange arrows refer to flexibility in timing of DOAC resumption after a procedure.
Antiplatelet agents
For all endoscopic procedures we recommend continuing aspirin (strong recommendation, low quality evidence), with the exception of ampullectomy (weak recommendation, low quality evidence). If considering aspirin discontinuation, this should be on an individual patient basis depending on the risks of thrombosis versus haemorrhage (weak recommendation, low quality evidence).
For low-risk endoscopic procedures we recommend continuing P2Y12 receptor antagonists as single or DAPT (strong recommendation, low quality evidence).
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing P2Y12 receptor antagonists 7 days before the procedure (strong recommendation, moderate quality evidence). In patients on DAPT, we recommend continuing aspirin (strong recommendation, low quality evidence).
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend continuing aspirin and liaising with a consultant interventional cardiologist about the risk/benefit of discontinuing P2Y12 receptor antagonists (strong recommendation, high quality evidence).
Aspirin
When given as long-term secondary prevention aspirin reduces vascular events by approximately one-third and vascular deaths by about one-sixth. In patients on long-term low-dose aspirin for secondary prevention, aspirin interruption was associated with a threefold increased risk of cardiovascular or cerebrovascular events, and 70% of these events occurred within 7–10 days after interruption.6 7 In a randomised controlled trial (RCT) of 220 patients on low-dose aspirin for secondary prevention undergoing non-cardiac surgery, patients were randomised to continuation or temporary replacement of aspirin by placebo.8 Major cardiac events occurred within 30 days in 1.8% of the aspirin group compared with 9% in the placebo group (p=0.02). No difference in haemorrhagic complications was seen between the two groups. The risks related to continuation or discontinuation of aspirin for endoscopy are discussed in the sections on endoscopic procedures, and recommendations made accordingly.
With regard to patients on a DOAC and a single antiplatelet agent, such as aspirin, the AFIRE trial randomised patients with atrial fibrillation (AF) and stable coronary artery disease to rivaroxaban alone versus rivaroxaban and a single antiplatelet. They demonstrated that rivaroxaban alone was non-inferior for the primary efficacy endpoint (a composite of thromboembolic events or death from any cause) and superior for the primary safety endpoint of major bleeding. However, this trial was not sufficiently powered to address the risk of stent thrombosis.9 For patients with documented coronary artery disease and an indication for formal anticoagulation, for example, AF, then a life-long single antiplatelet such as aspirin is no longer recommended, beyond the antiplatelet duration required postcoronary stent insertion, in the latest ESC guidelines.10 However, late stent thrombosis (1–12 months poststent implantation) and very late stent thrombosis (beyond 12 months poststent implantation) occur with a reported incidence of 0.5%–1.0% and 0.2%–0.4%, respectively, and stent thrombosis is associated with a 4%–45% mortality.11 Furthermore, technical aspects of the procedure, for example, left main stents, may have an essential bearing on the subsequent risk of stent thrombosis. The trials addressing whether a long-term antiplatelet agent is needed in patients that have stents and require a DOAC, which suggest a DOAC alone may be safe, are not sufficiently powered to look at the important endpoint of stent thrombosis.9 12 Many consultant interventional cardiologists in the UK recommend their patients remain on a single antiplatelet agent if they have stents and need a long term DOAC, although this will very much vary on an individual case-by-case basis. Therefore, in patients with coronary stents who are taking a DOAC the cessation of the single antiplatelet agent should always be discussed in advance with the consultant interventional cardiologist responsible for the patient’s care.
Following the publication of three RCTs in 2018 the use of aspirin in primary prevention in cardiovascular disease is no longer routinely recommended and should only be considered, on a case-by-case basis, in those with a very high individual risk of cardiovascular events.13
P2Y12 receptor antagonists
Antiplatelet drugs have a rapid onset of action, and irreversibly inhibit platelet activity. Clopidogrel, prasugrel and ticagrelor are antagonists of the P2Y12 receptor on platelets. Clopidogrel plus aspirin is more potent than aspirin alone.14 For clopidogrel, platelet function returns to normal 5–7 days after withdrawal of the drug.15 Prasugrel and ticagrelor are more rapidly acting and more potent platelet receptor antagonists than clopidogrel. Clopidogrel monotherapy may be used following a thromboembolic cerebrovascular accident, or for peripheral vascular disease. P2Y12 receptor antagonists are frequently used as DAPT with aspirin in acute coronary syndrome (ACS) and after placement of coronary stents. High-risk and low-risk indications for P2Y12 receptor antagonists are listed in table 2.
Patients on DAPT, with aspirin and a P2Y12 receptor antagonist, particularly in the context of coronary artery stents, are at high risk of thrombosis if drug therapy is discontinued. Without antiplatelet therapy coronary stents are at high risk of occlusion due to thrombosis, and this confers an approximate 40% risk of acute myocardial infarction or death. In one study, discontinuation of DAPT was associated with an HR of 161 for these events.16 DAPT is generally prescribed for 12 months after drug eluting stents (DES) implantation, though there have been occasional reported instances of thrombosis after this duration. Prasugrel and ticagrelor are now the main drugs of choice used for ACS in the UK. Prasugrel has been shown in a large UK observational series to be associated with a lower mortality.17 This has been confirmed in a large randomised open-label trial.18 The latest NICE guidelines for ACS now recommend prasugrel is used as the first line agent in ACS, unless the patient is on anticoagulant therapy, in which case clopidogrel is recommended. Clopidogrel is generally the first choice of P2Y12 inhibitor in patients undergoing elective percutaneous coronary intervention (PCI) and the current guidelines recommend a 6 month course of DAPT postelective PCI.10 Where temporary cessation of P2Y12 inhibitors in patients with stents has been agreed, after discussion with the responsible consultant interventional cardiologist, then stopping the P2Y12 inhibitors 7 days preprocedure will minimise the bleeding risk. However, it should be noted that, depending on the P2Y12 agent, this time can be shortened dependent on the P2Y12 agent in use. In patients with a very high risk of stent thrombosis there may also be a role for bridging either with intravenous cangrelor and/or GIIbIIIa agents. However, the role of such bridging agents is beyond the remit of this paper and this decision should be made along with the responsible consultant interventional cardiologist on a case-by-case basis.19
Bare metal stents (BMS), which only require 1 month of DAPT, are now much less frequently used and the national BCIS audit shows they are used in less than 15% of cases in the UK, and many units no longer even stock them. Their main indication is for use in patients with a high bleeding risk or requiring urgent major surgery. Many UK units now use BioFreedom DES, these are polymer-free drug coated stents, which have a license of 1 month of DAPT and are superior to BMS with respect to major safety endpoints including bleeding and restenosis rates.20 Finally, there is increasing evidence that with a number of third generation DESs 1 month of DAPT can safely be used in patients at high bleeding risk without an increase in ischaemic events.21–23 A single antiplatelet agent is continued in all cases after discontinuation of DAPT, this tends to be aspirin. In some cases, for example, patients who had a previous stroke, the patients may have aspirin stopped at the end of the DAPT course and clopidogrel continued long-term. The important issue of a single antiplatelet agent in patients on long-term DOACs is discussed in the previous section.
Finally, in patients on a DOAC for AF and stroke prophylaxis who need DAPT after stent implantation, evidence from trials such as the RE-DUAL trial indicate that much shorter courses of triple therapy followed by a course of DOAC and clopidogrel alone are safer than previous practice of triple therapy up to a year.24 The European Society of Cardiology and NICE guidelines, for both ACS and elective stenting, now support shorter durations of triple therapy followed by a DOAC and clopidogrel as the current standard of care.10 25 26
The duration of DAPT post-PCI may also depend on a number of other factors, beyond the scope of this guideline. Therefore, in patients with coronary stents, we recommend that the endoscopist discusses the plan, with respect to potential DAPT cessation, with a consultant interventional cardiologist. Ideally this should be the consultant interventional cardiologist responsible for the patient’s care, who did the stent procedure.
Anticoagulants
Warfarin and heparin
For low-risk endoscopic procedures we suggest that warfarin therapy should be continued (low quality evidence, moderate recommendation). It should be ensured that the INR does not exceed the therapeutic range in the week prior to the procedure (low quality evidence, strong recommendation).
Tell the patient to continue warfarin and check the INR during the week before the endoscopy.
If the INR result is within the therapeutic range then continue with the usual daily dose.
If the INR result is above the therapeutic range, but less than 5, then reduce the daily warfarin dose until the INR returns to within the therapeutic range.
If the INR is greater than 5 then defer the endoscopy and contact the anticoagulation clinic, or a medical practitioner, for advice.
For high-risk endoscopic procedures in patients at low thrombotic risk, we recommend discontinuing warfarin for 5 days before the procedure (strong recommendation, high quality evidence). Check INR prior to the procedure to ensure <1.5 (strong recommendation, low quality evidence).
Stop warfarin for 5 days before the endoscopy.
Check the INR prior to the procedure to ensure its value is <1.5.
On the day of the procedure restart warfarin with the usual daily dose that night.
Check INR 1 week later to ensure adequate anticoagulation.
For high-risk endoscopic procedures in patients at high thrombotic risk, we recommend that warfarin should be temporarily discontinued and substituted with LMWH (moderate quality evidence, strong recommendation).
Warfarin should be stopped for 5 days before the procedure.
Two days after stopping warfarin commence daily therapeutic dose of LMWH.
Administer the last dose of LMWH at least 24 hours prior to the procedure.
Check the INR prior to the procedure to ensure its value is <1.5.
Warfarin can be resumed on the day of the procedure with the usual dose that night.
Restart the daily therapeutic dose of LMWH on the day after the procedure.
Continue LMWH until a satisfactory INR is achieved.
Updated literature searches were conducted on the use of warfarin and heparin in patients undergoing endoscopy. There were no new data to indicate a change to the existing protocols above. Any new data relevant to interventional therapy are discussed in the sections on specific endoscopic procedures.
Direct oral anticoagulants
For low-risk endoscopic procedures we suggest omitting the morning dose of DOACs on the day of the procedure (weak recommendation, low quality evidence).
For high-risk endoscopic procedures in patients on DOACs, we recommend that the last dose of DOACs be taken 3 days before the procedure (strong recommendation. low quality evidence). For patients on dabigatran with a CrCl (or eGFR) of 30–50 mL/min we recommend that the last dose be taken 5 days prior to the procedure (strong recommendation, low quality evidence). In any patient with rapidly deteriorating renal function a haematologist should be consulted (strong recommendation, low quality evidence).
DOACs have been a major advance in anticoagulant therapy. Dabigatran is an inhibitor of thrombin, and rivaroxaban, apixaban and edoxaban inhibit FXa. They do not need routine monitoring, and INR and activated partial thromboplastin time (aPTT) are unreliable indicators of anticoagulant activity. Unlike warfarin they have a rapid onset of action and full anticoagulant activity is established within 3 hours of the first dose. They have relatively short half-lives, but these may be prolonged in renal failure, particularly for dabigatran. In patients undergoing a high-risk procedure with a low thrombotic risk we recommend that the last dose of rivaroxaban, apixaban or edoxaban is taken 3 days before the procedure. Dabigatran may have to be stopped for longer than this, however, when renal function is significantly reduced.27
For patients on dabigatran with CrCl of 30–50 mL/min we recommend that the last dose of the drug is 5 days before the procedure. Dabigatran therapy is contraindicated in patients with CrCl<30 mL/min. eGFR is a suitable alternative measurement of renal function, and the same numerical values apply for the purposes of these guidelines. If a patient on any DOAC is clinically deteriorating, his/her renal function should be checked before the procedure. These recommendations are supported by the findings of the PAUSE trial.5 Three thousand and seven patients on apixaban, dabigatran or rivaroxaban due for elective interventional procedures had a standardised interruption of therapy (figure 3): last dose of drug 2 days before low-risk procedures (including diagnostic GI endoscopy) and 3 days before high-risk procedures (including high-risk therapeutic GI endoscopy; eg, polypectomy). This was extended to last dose 5 days before a high-risk procedure for dabigatran patients with CrCL<50 mL/min. Resumption of therapy occurred at 1 day after low bleeding risk procedures and 2–3 days after high bleeding risk procedures. Low rates of major bleeding or arterial thromboembolism were observed. Low rates of venous thromboembolism were also observed although this was not a primary study outcome. We have maintained the recommendation to omit the morning dose of DOAC prior to low-risk endoscopic procedures, although the PAUSE trial demonstrates the safety of omitting the DOAC for 1 day before a low-risk endoscopic procedure if desired.
Bridging of anticoagulant therapy
Unfractionated heparin (UFH) and LMWH (LMWH) have short half lives compared with warfarin and can be employed as an anticoagulation ‘bridge’ while warfarin is temporarily discontinued for endoscopic procedures considered to have a significant risk of haemorrhage. UFH is administered by continuous intravenous infusion and LMWH by subcutaneous injection once or two times a day. The former requires an inpatient stay in hospital while warfarin is discontinued, and then re-introduced, and also requires frequent monitoring of aPTT; the latter can often be managed in an outpatient setting without monitoring of anticoagulation levels. Some cardiologists have a preference for UFH for bridging warfarin in patients with metal heart valves. A meta-analysis demonstrated higher rates of bleeding in patients with mechanical heart valves bridged with LMWH versus UFH, but numbers were small in the LMWH studies.28 A small multicentre registry study found no difference in adverse events between patients bridged with UFH or LMWH in this context,29 and bridging with LMWH is now commonplace. Guidelines from the American Heart Association and American College of Cardiology do not recommend one strategy over the other.30 Prosthetic metal heart valves in the mitral position are at particularly high risk of thrombosis if warfarin is temporarily discontinued for 5–7 days. Heparin bridging for patients with a bileaflet mechanical aortic valve replacement in the absence of AF is considered unnecessary in guidelines from the British Society of Haematology31 and from the American College of Cardiology/American Heart Association,32 but it is recommended in guidelines from the ESC and the European Association for Cardio-Thoracic Surgery.33 There are no high quality studies to inform us, and consequently levels of evidence are low quality in all three guidelines. We have now placed mechanical aortic valve replacement in the high-risk category requiring bridging, in line with European guidelines, but this should be decided in conjunction with local cardiology or cardiothoracic surgery services given the uncertainty. This should always be discussed with the consultant cardiologist responsible for the patient’s care.
The risk of thromboembolism with AF increases with additional cardiovascular factors such as hypertension, heart failure and diabetes and this risk has been quantified by the CHADS2 score (annual risk of stroke increasing from 1.9% with a score of 1 to 18.2% with a score of 6). This has been updated with the CHA2DS2VASc scoring system in which the annual risk of stroke increases from 1.3% with a score of 1 to 15.2% with score of 9. A randomised, prospective, double-blind placebo-controlled trial was conducted in 1884 patients with AF undergoing a variety of operative procedures including approximately 50% GI endoscopy.34 Patients were randomised to LMWH or placebo, and risk factors were well matched. Thirty-eight per cent of the patients had CHADS2 scores>3, <2% had mitral stenosis and ≤3.4% had CHADS2 scores of 5 or 6. There was no significant difference in rates of thromboembolism between the LMWH and placebo groups, but there was a significant increase in major haemorrhagic events in the LMWH group versus placebo (3.2% vs 1.3%). Caution should be exercised when interpreting the results in the high-risk thromboembolic groups as the study was not designed or statistically powered to examine these categories. The previous BSG/ESGE guidelines1 do not recommend bridging for non-valvular AF, ASGE guidelines35 recommend bridging with LMWH for CHA2DS2VASc>2 and the APAGE/APSDE guidelines36 recommend this for CHA2DS2VASc>5. CHADS2 scores are unfortunately not directly equivalent to CHA2DS2VASc scores. Further research on the benefits of heparin bridging is required in high-risk patients with non-valvular AF on warfarin in order to determine the optimum approach, but it would be reasonable to consider bridging patients with CHADS2 scores >5 as recommended by the British Society of Haematology.31 This applies to patients with AF and a previous stroke or transient ischaemic attack (TIA), and three of the following factors: congestive cardiac failure, hypertension (>140/90 mm Hg or on antihypertensive medication), age>75 years or diabetes mellitus. Heparin bridging is also recommended for patients with AF who have had a stroke or TIA within 3 months.31
Bridging with LMWH has also been studied in patients on DOACs. In a German registry, heparin bridging versus no bridging led to a higher rate of major haemorrhage (2.7% vs 0.5%, p=0.01) with no reduction in thromboembolism.37 In the RE-LY trial bridging of dabigatran with LMWH resulted in higher major haemorrhage rates compared with no bridging (6.5% vs 1.8%, p<0.001) with no difference in thrombosis rates between the groups.38
In a Japanese study of 16 977 patients on warfarin or DOACs undergoing a variety of high-risk endoscopy procedures a propensity matched analysis demonstrated a significant increase in postprocedure GI bleeding and thromboembolism in patients who were bridged with heparin.39 It should be noted that all patients were bridged with UFH rather than LMWH. For colonoscopy in patients on warfarin who were bridged with LMWH, several studies have demonstrated an increase in postpolypectomy haemorrhage without a decrease in thromboembolic events.40–42 Bridging with LMWH should, of course still be advocated for those patients on warfarin at high risk of thromboembolism (table 3), but patients should be advised of the increased risk of post-procedure haemorrhage. The safety of temporary cessation of DOAC therapy, without bridging, is supported by the findings of the PAUSE trial.5
Patients with a history of venous thromboembolism within 3 months of commencing anticoagulant therapy are at high risk of recurrent thrombosis if anticoagulation is interrupted. Most of these patients are now commenced on a DOAC rather than warfarin, and bridging would not be recommended. Ideally we should not interrupt anticoagulation in this high-risk group due to the risk of thrombosis; an elective low-risk procedure could be performed without interrupting anticoagulation if necessary, but it may be preferable to defer a high-risk procedure beyond 3 months anticoagulation if safe to do so.
Patients with thrombophilia syndromes should be discussed with a haematologist. Factor V Leiden and the common prothrombin mutation F2G20210A are low-risk thrombophilias and bridging is not required. Patients with deficiencies of antithrombin, protein C or protein S are at higher risk of thrombosis, but in most of these patients bridging therapy will not be required.
Endoscopic procedures
Minor haemorrhage is not uncommon during therapeutic endoscopic procedures, but we have considered it to be clinically significant when haemoglobin value falls by more than 20 g/L, necessitates blood transfusion, or causes an unplanned hospital admission. Haemorrhage may be apparent at the time of endoscopy, or delayed up to 2 weeks following the procedure. For those in whom antithrombotic therapy is interrupted, the latter situation presents a higher risk, as therapy will usually have been recommenced within that period. There are relatively few studies of the risks of haemorrhage for endoscopic procedures in patients who continue antithrombotic therapy, therefore, much of the data underlying the risk levels for these procedures applies to the baseline risk of haemorrhage without antithrombotic therapy (table 3).
Diagnostic endoscopy and mucosal biopsy
Diagnostic endoscopies, including mucosal biopsy sampling, confer a minimal risk of haemorrhage, and no severe haemorrhage has been reported in studies involving thousands of patients in total.43–47 No increased risk of haemorrhage from biopsy has been found in studies of patients on aspirin, clopidogrel or warfarin.48 49 A prospective case–control study of patients taking antiplatelet or anticoagulant drugs, including DOACs, found no incidence of significant bleeding in either the antithrombotic or control group who had upper GI biopsies taken.50 Only 19 of the 277 patients who continued antithrombotics were on DOACs. The approximate mean number of biopsies per patient was only two in either group in this study, and in all the above studies only small numbers of biopsies were taken. In a prospective registry study 119 patients were identified who had continuation of DOAC for endoscopy, and 29 patients had biopsies on continued DOAC.51 There were two cases of non-major clinically significant haemorrhage and no cases of major haemorrhage. There is one case report of life-threatening bleeding following multiple biopsies for Barretts oesophagus in a patient on aspirin who was later found to have high grade dysplasia.52 A prospective study of endoscopic practice in Italy53 regarding adherence to the previous BSG/ESGE antithrombotic guidelines1 found an increased incidence of haemorrhage in patients undergoing mucosal biopsies in whom DOAC therapy was continued compared with those in whom the morning dose was withheld as recommended in the guidelines (2/38 5.2% vs 2/114 1.7%, respectively). However, numbers of cases were small, the study was not adequately powered to determine this issue, and the difference did not reach statistical significance.
The pharmacokinetic profile, and hence pharmacodynamic effect, of DOACs varies such that some individuals will have higher peak levels 2–6 hours after oral administration.54 Consequently, at the time of an endoscopic biopsy the anticoagulant effect due to a DOAC is not accurately predictable. Due to this uncertainty regarding the level of anticoagulation on DOACs at the time of endoscopy, and the absence of reliable test of anticoagulation on these drugs, we continue to suggest omitting the dose of DOAC on the morning of the procedure to allow an adequate safety margin. This applies to both once a day and two times a day regimens.
Resection of GI polyps
Polypectomy including endoscopic mucosal resection
Studies of colonoscopic polypectomy have identified a risk of postpolypectomy bleeding (PPB) of 0.07%–1.7%.47 55–58 It is important to differentiate between immediate and delayed PPB, and also to identify the severity of bleeding; these factors are not always clear in the literature. Delayed PPB is of particular importance in patients in whom antithrombotic therapy has been interrupted, as bleeding will often occur once antithrombotics have been restarted. In a BSG audit of 20 085 colonoscopies in the UK, 52 (0.26%) haemorrhages were reported, but only 3 (0.01%) were major.59 Data from the English National Bowel Cancer Screening Programme found an overall PPB rate of 1.14%, with a rate of severe bleeding requiring transfusion of 0.08%.60
Risk factors for PPB include polyp size61 use of pure cutting current62 and use of a non-microprocessor-controlled current for endoscopic mucosal resection (EMR).63 Use of endoscopic clips or submucosal injection of diluted epinephrine may also reduce the risk of PPB,64 65 Caution is advised, however, when using clips prior to excision for pedunculated polyps as one RCT was closed prematurely due to complications: one perforation (1.5%) and three mucosal burns (4.5%).66 An RCT of cold-snare versus hot-snare polypectomy (341 vs 346 polyps, respectively) of polyps 4–9 mm demonstrated no significant haemorrhage in the cold-snare group.67 In all of these studies, patients on antiplatelet therapy or anticoagulation were excluded.
A number of studies have examined the risks of resection of small colonic polyps on continued antitcoagulant therapy. A single centre case series of 1177 cold snare polypectomies compared PPB in those on antiplatelets or anticoagulants compared with those not on these drugs.68 There was an increase in immediate bleeding, mostly in warfarin patients, but no significant difference in delayed bleeding (up to 2 weeks) between the groups. A retrospective study of 223 polypectomies (<1 cm, with or without diathermy) in 123 patients on continued warfarin therapy found a rate of haemorrhage requiring transfusion of 0.8%. This was despite routine prophylactic clipping of polypectomies.69 In an RCT (159 polyps <1 cm in 70 patients) examining hot versus cold snaring of polyps in anticoagulated patients, the rate of immediate haemorrhage in the hot snare versus the cold snare group was 23.0% versus 5.7%, respectively, and that of delayed haemorrhage requiring intervention 14% versus 0%, respectively.70 An RCT compared cold polypectomy <1 cm in patients on DOAC or warfarin bridged with UFH compared with cold polypectomy on continued anticoagulant.71 The incidence of polypectomy-related major bleeding was high at 12.0% in the former group and 4.7% in the latter. The majority of patients in the study would not have not have been considered for bridging by British Society of Haematology guidelines,31 and LMWH would have been recommended for any that did qualify for bridging.
The risk of polypectomy on continued antiplatelet therapy has also been studied. Aspirin monotherapy has been found to be safe in colonoscopic polypectomy.72–74 A double blind RCT included patients on clopidogrel therapy who required colonoscopy.75 They were randomised at 7 days before procedure into either continuing with clopidogrel 75 mg a day or placebo until the morning of colonoscopy. If discontinued, clopidogrel was restarted after colonoscopy when oral intake was allowed. More than 90% of patients had polyps les than 1 cm. There was no significant difference in immediate or delayed PPB, or in cardiothrombotic events, between the two groups. These conclusions, however, need to be treated with some caution. Although the study aim was to examine the effect of clopidogrel, a high proportion of patients were on DAPT. The groups were well matched but numbers were relatively small to examine differences in an infrequent event, and the rate of PPB in the placebo group was higher than expected when compared with other studies of patients undergoing polypectomy not previously on antiplatelet agents. A meta-analysis76 assessing the risks of immediate and PPB associated with continued clopidogrel use at time of polypectomy included the above trial. A total of five studies were identified which included 655 patients in the ‘continuing clopidogrel’ group and 6620 controls with interrupted clopidogrel therapy. There was an increased risk of PPB in the continuing clopidogrel group (risk ratio 1.96; 95% CI 1.36 to 2.83; p=0.0003). There was no significant difference in serious cardio thrombotic events occurring within 30 days of the procedure. In the above studies the great majority of polypectomies were <1 cm. Further research is required, particularly with respect to polypectomy on DAPT, but based on the above data, it may be safe to undertake polypectomy for polyps <1 cm in size on clopidogrel monotherapy. To minimise the risk of PPB cold snare polypectomy may be advisable. Alternatively, temporarily substituting aspirin for clopidogrel may be desirable 7 days prior to colonoscopy.
In large case series of EMR, the incidence of immediate and delayed bleeding ranged between 3.7%–11.3% and 0.6%–6.2%, respectively.63 77 78 For EMR of small lesions (<1 cm), however, PPB rates were similar to those reported following conventional polypectomy.78 A retrospective cohort study did not find aspirin (continued till day of procedure) or P2Y12 receptor antagonists (stopped 5–7 days before EMR) to be significant factors associated with bleeding post-EMR of colon neoplasia.79 However, only a small minority (aspirin 20% and clopidogrel 2%) of patients were taking these medications. The rate of delayed post-EMR bleeding in the oesophagus is low (0.6%–0.9%), even in studies that include a high proportion of patients with a temporary cessation of antiplatelet therapy.80 81 In two retrospective observational studies of duodenal EMR, delayed bleeding was reported in 14/113 (12.3%)82 and 7/111 patients (6.3%)80 despite the prophylactic use of endoclips in 82% of cases in the latter. There are conflicting studies on the use of prophylactic endoclips for EMR.83–85 A cost-efficacy analysis concluded that prophylactic placement of endoscopic clips after polypectomy was a cost-effective strategy for patients receiving antiplatelet or anticoagulation therapy.86 Prophylactic use of endoclips may therefore be advisable for EMR in patients on antithrombotics due to the increased risk of PPB.
Endoscopic submucosal dissection
There have been several studies of endoscopic submucosal dissection (ESD) on continuous low dose aspirin since the previous version of this guideline. One retrospective multicentre study87 for colonic ESD, and six retrospective studies of gastric ESD,88–93 comparing continuation with interruption of aspirin, found no significant differences in delayed bleeding the two groups. This was confirmed by two meta-analyses which also reported that continuation of low dose aspirin does not increase the postprocedure bleeding after ESD.94 95 This was also observed in the group of patients under DAPT in which aspirin was continued alone.88 Furthermore, inappropriate discontinuation of antiplatelet agents was significantly associated with increased risk of thrombosis.90 A meta-analysis found a thrombosis rate of 2.1% in the aspirin-interrupted versus none in the aspirin-continued group of patients.95
Continued thienopyridine (clopidogrel or prasugrel) or aspirin use did not increase delayed haemorrhage for gastric ESD in one retrospective study.92 A non-randomised retrospective comparative study found, however, that continuation of any antithrombotic, or heparin bridging, increased the risk of haemorrage with gastric ESD.93 The risk of haemorrhage following gastric ESD is increased with the number of antiplatelet agents taken or when antiplatelet drugs are combined with anticoagulation.96 For colorectal ESD, antiplatelet agents except for aspirin alone were independent risk factors of delayed bleeding (OR 4.04, 95% CI 1.44 to 11.30, p=0.008) in a retrospective multicentre study including 180/1189 patients on antiplatelets.87
In a large national database including 16 977 patients who underwent high-risk endoscopic procedures under oral anticoagulation, upper and lower GI ESD were found to be significantly associated with postprocedure haemorrhage.39 The delayed bleeding rate after ESD at any location has been found to be 16% in patients who have had warfarin or DOACs, including those with heparin bridging (UFH).97 A meta-analysis of ESD studies found a significant increase in delayed haemorrhage and an increase in thrombosis with heparin bridging compared with those who discontinued anticoagulation without bridging.94 A meta-analysis focused on heparin bridging therapy (UFH) for gastric ESD patients on warfarin or DOACs found an increased risk of haemorrhage without any benefit in thrombosis.95 Studies of colonic ESD on anticoagulants have included small numbers and retrospective analysis, and conflicting conclusions have been derived.87 98 99 Few data are available for oesophageal or duodenal ESD on antithrombotics. The risk of bleeding after oesophageal ESD is lower at compared with other locations,100 101 but one retrospective study found a significant higher readmission rate after oesophageal ESD for patients with a history of antiplatelet or anticoagulant use (56.4% vs 34.1%; p=0.01).102
Several methods have been proposed to reduce the risk of haemorrhage after ESD including pharmacological (PPI), mechanical (clips, endoscopic hand sutures) and local topical (fibrin glue and polyglycolic acid sheets, haemostatic powder) techniques, and these should be particularly considered in patients on antithrombotic therapy.
Endoscopic retrograde cholangiopancreatography
In a meta-analysis (21 prospective studies; 16 855 patients), the overall haemorrhage rate following endoscopic retrograde cholangiopancreatography (ERCP) was 1.3%, with 71% of these being graded as moderate and 29% as severe; the mortality rate was 0.05% overall.103 Post-ERCP haemorrhage is most frequently seen after endoscopic biliary sphincterotomy. An ESGE guideline on ERCP-related adverse events has suggested that patients should be considered to be at increased risk for post-sphincterotomy haemorrhage if at least one of the following factors is present: anticoagulant intake, platelet count <50 x10ˆ9/L, cirrhosis, dialysis for end-stage renal disease, intraprocedural bleeding and low endoscopist experience.104 There are a number of measures which can reduce the risk of haemorrhage at ERCP including avoidance of sphincterotomy prior to biliary stenting,105 and use of a blended current rather than pure-cutting current.106–108 These, and other measures to reduce the risk of haemorrhage are discussed in previous ESGE guidelines.104 105
Two uncontrolled retrospective studies reported post-endoscopic sphincterotomy (ES) bleeding in 8 (19%) of 43 patients under antiplatelet monotherapy or dual therapy, including only one significant episode of haemorrhage.109 110 Controlled studies of bleeding following ES performed under antiplatelet therapy have failed to demonstrate an increase in patients taking antiplatelets at the time of ES versus controls, but studies were underpowered to show a difference.110–112 A single retrospective study (762 patients) has compared post-ES bleeding rates in patients who discontinued antiplatelets for >7 days (n=29), <7 days (n=83) or did not discontinue antiplatelets (n=49).111 The incidence of bleeding (defined as clinical evidence of bleeding or a drop in haemoglobin>20g/L) was respectively 10.3% (delayed, 6.9%), 6.0% (delayed, 2.4%) and 16.3% (delayed, 14.3%). The only significant association was between sustained antiplatelet use and the delayed type of post-ES bleeding. Of note, a majority of antiplatelet users were taking aspirin only. A retrospective study in which 50/191 patients undergoing ES were on aspirin, showed no statistically significant increase in haemorrhage in the aspirin group.113 Haemorrhage following endoscopic sphincteroplasty has been reported in 0%–8.6% of patients.114 One small case series suggested that continued aspirin therapy may be safe,115 but there are no data on other antithrombotics. There are no data for biliary mechanical lithotripsy, cholangioscopy or electrohydraulic lithotripsy therapy in patients taking antiplatelets or anticoagulants.
Ampullectomy
A meta-analysis (29 studies, 1751 patients) reported that haemorrhage occurs in 10.6% of ampullectomies with approximately 25% and 5% requiring blood transfusion and non-conservative management, respectively.116 Various measures to prevent haemorrhage have been studied, but more research is required to make definitive conclusions. A non-randomised pilot study (n=80) suggested that routinely closing the mucosal defect with clips following ampullectomy is effective to prevent delayed bleeding (5% vs 22.5%, p=0.026).117 An RCT has suggested that, compared with the autocut mode, the endocut mode may prevent immediate but not delayed bleeding in cases with tumours>14 mm; it causes more frequent crush artefacts.118 Prophylactic argon plasma coagulation has been reported as effective in a retrospective study (n=82) and ineffective in an RCT (n=54) to prevent post-ampullectomy bleeding.119 120 Submucosal injection prior to ampullectomy did not prevent bleeding in an RCT (n=50) and a retrospective matched cohort analysis (n=50)121 122; furthermore it was associated with higher tumour recurrence rate and a shorter recurrence-free survival in the retrospective study.121 There are no data on ampullectomy on anticoagulants or P2Y12 receptor antagonists as these are usually withdrawn. Given the high haemorrhage rate, withdrawal of aspirin should be considered on an individual basis depending on the risks of thrombosis.
Endoscopic ultrasound-guided with fine-needle aspiration, and other interventions
The incidence of haemorrhage following endoscopic ultrasound (EUS)-guided sampling has been analysed in several systematic reviews; the figure per thousand was 1.28 for EUS-guided with fine-needle aspiration (FNA) (51 studies, 10 941 patients),123 5.81 for EUS-fine needle biopsy (FNB) (51 studies, 5330 patients)124 and 6.63 for EUS-FNA of pancreatic cystic lesions (40 studies, 5124 patients).125 Four studies reported on haemorrhage following EUS-guided sampling in patients prescribed antithrombotic agents.126–129 The only significant differences were between patients on prophylactic LMWH and controls.128 In the largest study, however, no severe haemorrhage was found in patients who continued or discontinued antithrombotic therapy, and only one thromboembolic event occurred.129
EUS-guided biliary drainage, an alternative to ERCP-guided biliary stenting, has been suggested to be safely feasible in patients with sustained use of antiplatelets and/or anticoagulants. In a retrospective study that included 41 patients on antiplatelets and/or anticoagulants (23 patients under DAPT, anticoagulant or a combination of antiplatelet and anticoagulant) and 154 controls, bleeding rates were not significantly different in the antiplatelet/anticoagulants and control groups (7.3% and 2.6%, respectively).130 The safety of EUS-guided biliary drainage should however be confirmed in prospective studies, adequately powered to evidence a significant difference, before a recommendation can be made. Invasive therapeutic procedures such as EUS and cystgastrostomy or necrosectomy have a significant risk of major haemorrhage and should be considered as high risk for P2Y12 receptor antagonists or anticoagulants. The risk on aspirin is unknown.
Endoscopic dilatation
Review of studies which included greater than 100 patients with benign upper GI strictures, either anastomotic, achalasia, post-ESD, eosinophilic, gastric outlet obstruction or mixed aetiology, reveals a risk of haemorrhage well below 1%.131–140 A systematic review and meta-analysis of studies of endoscopic dilatation of gastroduodenal Crohn’s disease strictures revealed a 2.1% per procedure risk of haemorrhage.141 In a prospective study of dilatation in 55 patients with oesophageal carcinoma no clinically relevant haemorrhage was observed.142 Dilatation for lower GI strictures, either iatrogenic or related to inflammatory bowel disease, revealed no significant haemorrhage in prospective studies or larger retrospective case series (over 100 patients).143–147 No data were found regarding dilatation in malignant colonic strictures.
A study of the complications arising from 504 balloon dilations in 237 patients with achalasia revealed 4 (1.7%) asymptomatic haematomas, but no clinically significant haemorrhage.148 There were, however, 7 (3%) perforations. In an RCT of pneumatic dilatation versus laparoscopic myotomy for achalasia there were no reported haemorrhages but 8/108 (9.5%) patients experienced perforation during the treatment course.149
Dilatation of GI strictures in the upper or lower GI tract appears to be a low-risk procedure, with the exception of Crohn’s disease-related ileal strictures, and balloon dilatation for achalasia. There are no data, however, on dilatation of strictures on antiplatelets or anticoagulants. This, together with the inaccessibility of the site of haemorrhage for endoscopic haemostasis, has led us to continue to consider endoscopic dilatation as a high-risk procedure on P2Y12 receptor antagonists or anticoagulants.
Endoscopic stenting
There are no studies on endoscopic stenting at any site in the GI tract in patients taking antiplatelets or anticoagulants. Available data regarding haemorrhage risk, from RCTs, prospective and mostly retrospective studies, are heterogeneous regarding details of the time interval from stent placement until clinically relevant haemorrhage occurred, In deciding whether stent insertion is a high or low-risk procedure we considered haemorrhage within 7 days of insertion.
Previous reviews of risks associated with endoscopic stent insertion have been confounded by the variety of stents used and the evolution of stent design with time. With respect to oesophageal self-expanding metal stents (SEMS), eight recent studies of demonstrated a risk of 0% significant haemorrhage within 7 days of insertion.150–157 However, studies including delayed haemorrhage showed a risk of 9% in an RCT comparing small-diameter stents with large-diameter stents and an 8% risk in a large retrospective series of 997 patients.158 159 Causes of haemorrhage included aorta-oesophageal fistula formation, and continued oozing from tumours.154 160
With respect to duodenal SEMS, large (>100 patients) and recent retrospective and prospective studies showed a haemorrhage risk within 7 days of less than 1%.161–163 The one exception was a retrospective study including 152 patients, whereby the safety and benefits of SEMS combined with chemotherapy were investigated: in total 4 patients (2.6%) suffered from haemorrhage that requiring blood transfusion. Though none of these patients had concomitant chemotherapy, two-thirds had coexisting biliary obstruction for which an intervention was simultaneously performed.164
With respect to colonic SEMS, a large prospective series of 513 patients and 6 retrospective studies found the risk of clinically relevant haemorrhage within 7 days to be 0%.165–174 A systematic review identifying 40 studies on SEMS for the management of emergency malignant large bowel obstruction identified 9 studies reporting on clinical relevant bleeding which occurred in 0.5% (8 out of 1474 patients).175
We have considered endoscopic stenting at all sites in the GI tract to be low risk for haemorrhage within 7 days. Patients on antithrombotics may be at increased risk of delayed haemorrhage, however.
Percutaneous endoscopic gastrostomy
Minor haemorrhage around the wound site at percutaneous endoscopic gastrostomy (PEG) placement is usually short-lived. Severe haemorrhage is rare, and may be secondary to PEG tract bleeding, injuries to the gastric artery, splenic or mesenteric vein (massive retroperitoneal bleeding), or rectus sheath haematoma.176–178 Rarely, laparotomy may be required as a result of puncturing of the gastric artery at the time of insertion.177
The overall risk of haemorrhage for PEG placement was 1.5% in a case series of 950 patients.179 There are few data on continued administration of antithrombotics at the time of PEG insertion. A meta-analysis showed continuing antiplatelet therapy such as clopidogrel may be safe.180 A German retrospective study of PEG insertion with patients on UFH, phenprocoumon, LMWH, aspirin, clopidogrel and combinations showed no evidence of increased haemorrhage.181 A further study concluded that giving aspirin or clopidogrel either 72 hours before or 48 hours after the procedure did not increase bleeding risk.182 The above studies are, however, of inadequate quality to definitively demonstrate an effect due to the drugs studied. A large retrospective study of patients undergoing endoscopic procedures on anticoagulants included 2322 PEG performed on warfarin and 1484 on DOACs, with a risk of post-endoscopy bleeding of 2.0% and 1.2%, respectively.39
Device-assisted enteroscopy
Single-balloon, double-balloon and spiral enteroscopy devices are available. The risk of haemorrhage from enteroscopy has been reported at 0.2%–0.3%.183 184 Spiral enteroscopy was not associated with a risk of clinically significant haemorrhage in a small case series.185 Double balloon enteroscopy is associated with a perforation rate of 0.1%–0.4%183 186 and this rises to 1.5% if polypectomy is performed.186 In a retrospective single centre study of 420 patients undergoing double-balloon enteroscopy, it was noted that 13% were on anticoagulation.187 Although the risk of bleeding may be low for diagnostic procedures, therapeutic procedure such as polypectomy would confer a high risk of haemorrhage on antithrombotics. Endoscopic therapy was performed in 47.1% of 257 double-balloon procedures in a UK case series.188
Oesophageal variceal banding
Generally, variceal band ligation (VBL) is undertaken when there is recent or active bleeding. However, elective variceal banding may be necessary at surveillance. In a case–control study of bleeding following VBL 3.4% of patients had haemorrhage secondary to banding induced ulcerations.189 In a study of 605 patients undergoing VBL, 21 (3.5%) patients had spontaneous bleeding due to band slippages confirmed at endoscopy and 11 died.189 Multivariate analysis found no increased risk of bleeding in those on aspirin, although this applied to only 8/605 patients
A study of planned VBL in cirrhotic patients, including 265 patients on LMWH, showed no increase in post-procedural haemorrhage or reduction in survival compared with those not on LMWH.190 An uncontrolled case series of five patients undergoing elective VBL on continued warfarin observed no post-banding haemorrhage.191 Placing no more than six bands per session may help reduce the risk of post-banding ulcer haemorrhage.192 In a large retrospective series, the risk of haemorrhage in patients undergoing variceal banding on DOAC or warfarin was high for both groups at 19.2% and 25.9%, respectively p=0.49.39 There are no studies of VBL in patients on P2Y12 receptor antagonists.
Ablative therapies
Radiofrequency ablation (RFA) in the oesophagus is a well-established treatment for dysplasia within Barretts oesophagus. A meta-analysis of studies of oesophageal RFA has found a rate of haemorrhage of 1%.193 RFA has been used to treat gastric antral vascular ectasia, but we have only small case studies to inform us, as demonstrated in a systematic review.194 In one case series of 21 patients there was a 10% ulceration rate necessitating discontinuation of RFA therapy. We have therefore classified oesophageal and gastric RFA as high risk for haemorrhage with respect to P2Y12 receptor antagonists and anticoagulants. There are no data on aspirin, but we advise continuation in other procedures with similar rates of haemorrhage.
Argon plasma coagulation is used as an ablative therapy for a wide variety of indications throughout the GI tract, including ablation of vascular abnormalities including angiodysplasia and radiation proctitis, ablation of tumours and margins of resected polyps, ablation of dysplastic Barretts oesophagus, and occasionally as a haemostatic measure. With different indications there is variation in size of the ablated mucosal field, energy delivered, and consequences including rarely perforation. There are no data on continued use of antithrombotics with respect to the risk of haemorrhage from APC, and we are therefore unable to provide specific guidance in this regard.
Restarting antithrombotic therapy for elective procedures
There are few data to inform us on the optimal time to restart antithrombotic therapy, if discontinued, after elective endoscopic therapy. Decisions in all cases will be based on the perceived risk of haemorrhage following the procedure versus the risk of thrombosis to an individual patient. It should be remembered that DOACs exert an anticoagulant effect within hours, compared with days for warfarin. Data from the PAUSE study indicates that restarting a DOAC 2–3 days after a high-risk procedure has a low risk of thromboembolic events.5 Data on restarting therapy after acute GI haemorrhage are discussed in that section. A prospective cohort study in Italy53 evaluated the risks of haemorrhage and thrombosis in relation to compliance with the previous version of this BSG/ESGE guideline. For cases who underwent polypectomy there was a trend to more intraprocedural bleeding if DOAC was not stopped as per the guideline for high-risk procedures. Stopping longer than the guidelines did not reduce the intraprocedural bleeding risk. Also, restarting the DOAC immediately after polypectomy, rather than a delay of 24–48 hours (as suggested by the guidelines) in high-risk patients led to an almost doubling of the delayed bleeding risk without a reduction in thrombosis, although these measures did not reach statistical significance.
For procedures with a very high risk of haemorrhage such as ESD, it may be desirable to delay restarting antithrombotics beyond the intervals recommended in these guidelines. In a meta-analysis, post-ESD bleeding risk was not significantly increased if antithrombotic therapy was resumed at least 1 week after ESD whereas resumption of antithrombotic therapy immediately or within 1 week after ESD was significantly associated with post-ESD bleeding.94 The incidence of thrombosis was not analysed, however, and this needs to be considered on an individual patient basis.
Risk stratification for elective endoscopic procedures
Endoscopic procedures carry a higher risk of haemorrhage, and certain clinical situations will result in a high risk of thromboembolic complications should antiplatelets or anticoagulants be withdrawn. Procedures have been classified as high-risk or low-risk for haemorrhage primarily based on the risks of haemorrhage in patients not taking antiplatelets or anticoagulants, as well as some limited data available regarding endoscopy in patients in whom these drugs were continued (table 1). Tables 2 and 3 stratify risk for discontinuation of P2Y12 receptor antagonists or warfarin respectively according to clinical scenario, and the risks of thromboembolic sequelae on discontinuation of therapy.
Diagnostic endoscopic procedures, with or without biopsy, are classified as low-risk for haemorrhage, though there is concern regarding biopsy on DOACs. The likelihood of having to undertake therapy with a risk of haemorrhage should also be considered, for example, colonoscopy when polyps have been found in 22.5%–34.2% of patients in large studies.47 55 Endoscopists may therefore choose to manage colonoscopies as high-risk procedures with respect to P2Y12 receptor antagonists and anticoagulants. Similar considerations apply to ERCP if there is uncertainty as to whether sphincterotomy will be required.
Acute GI haemorrhage on antiplatelets and anticoagulants
Antiplatelets
We suggest that permanent discontinuation of aspirin for primary prophylaxis should be considered (weak recommendation, low quality evidence).
We suggest that aspirin for secondary prevention should not be routinely stopped. If it is stopped, it should be recommenced as soon as haemostasis is achieved, or there is no further evidence of bleeding (strong recommendation, moderate quality evidence).
We recommend that DAPT is continued if possible in patients with coronary stents in situ and management should be in liaison with a consultant interventional cardiologist (strong recommendation, moderate quality evidence). In the case of major haemorrhage we recommend continuing aspirin if the P2Y12 receptor antagonist is interrupted (strong recommendation, moderate quality evidence). P2Y12 receptor antagonist therapy should be re-instated within 5 days, if still indicated (strong recommendation, moderate quality evidence).
Antiplatelets confer an increased risk of spontaneous haemorrhage, but also present an increased risk to the patient when this occurs. In the case of life-threatening haemorrhage, this is of urgent concern, but withdrawal of antiplatelet therapy confers a risk of thrombosis. A meta-analysis of studies of patients on aspirin for secondary prophylaxis found that discontinuation of aspirin was associated with a threefold increased risk of major adverse cardiac events, increasing to an OR of 89 for major cardiac events in patients with coronary stents.6 If GI haemorrhage occurs in a patient with a recently placed coronary stent on DAPT, then life-threatening thrombosis could occur if therapy is interrupted. The imperative, after adequate resuscitation, is to achieve haemostasis within the GI tract and urgent facilities should be available to provide this. Liaison with a consultant interventional cardiologist should occur in the emergency setting. If it is deemed necessary to temporarily discontinue antiplatelet therapy, this should be limited to the P2Y12 receptor antagonist, and aspirin continued.195 The timing of restarting antithrombotic therapy after acute GI haemorrhage will be determined by the risk of re-bleeding and the risk of acute thrombosis without antithrombotic therapy.196 P2Y12 receptor antagonists in patients with coronary stents should be restarted within a maximum of 5 days due to the high risk of stent thrombosis after this time. This timeframe represents an optimal balance between haemorrhage and thrombosis,195 though it has not been tested prospectively.
For patients on aspirin monotherapy for secondary prophylaxis, there is a benefit to continued therapy. A prospective placebo-controlled RCT of 156 patients following endoscopically controlled upper GI haemorrhage, demonstrated a reduction in all-cause mortality in the group receiving low-dose aspirin (1.3% vs 12.9%).197 There was an excess of bleeds in the aspirin group (10.3% vs 5.4%) but none were fatal. Five patients in the placebo arm died of thromboembolic events. If aspirin is stopped then it should be reintroduced as soon as haemostasis has been achieved.
A retrospective study of 118 patients on antiplatelets or anticoagulants presenting with acute GI haemorrhage compared outcomes in those who had antithrombotic therapy permanently discontinued compared with those in whom it was restarted.198 In those in whom antithrombotic therapy was discontinued the HR for thrombotic events was 5.77 (95% CI 1.26 to 26.35) and for mortality 3.32 (1.07–10.31) compared with those in whom it was restarted. It is therefore important to have a plan for consideration of restarting antithrombotic therapy in all such patients presenting with GI haemorrhage.
Anticoagulants
We recommend withholding oral anticoagulant and correcting coagulopathy according to the severity of haemorrhage and the patient’s thrombotic risk in coordination with a consultant cardiologist/haematologist. The correction of coagulopathy should not delay endoscopy or radiological intervention (strong recommendation, low quality evidence).
In patients with haemodynamic instability who take VKAs, we recommend administering intravenous vitamin K and four-factor PCC (strong recommendation, low quality evidence), or fresh frozen plasma if PCC is not available (weak recommendation, very low quality evidence)
In patients with haemodynamic instability who take DOACs, we suggest considering the use of reversal agents: idarucizumab in dabigatran patients, and andexanet in anti-FXa treated patients (weak recommendation, low quality evidence), or intravenous four-factor PCC if andexanet is not available (weak recommendation, very low quality evidence).
We recommend restarting anticoagulation following acute GI haemorrhage in patients with an indication for long-term anticoagulation (strong recommendation, low quality evidence). In patients at low thrombotic risk, we suggest restarting anticoagulation as soon as possible after 7 days of anticoagulant interruption (weak recommendation, low quality evidence). In those at high-thrombotic risk, an earlier resumption of anticoagulation with heparin bridging, preferably within 3 days, is recommended (strong recommendation, low quality evidence).
Anticoagulant use is reported in up to 15% and 25% of patients presenting with acute upper and lower GI bleeding, respectively.199–201 GI bleeding-related mortality in these patients is high (up to 8%–12%), but mainly related to patients’ comorbidities. Anticoagulants are independent predictors of neither mortality nor in-hospital rebleeding,202–205 provided they are managed appropriately. Temporary discontinuation of anticoagulation is the ‘standard of care’ in patients with clinically significant GI bleeding.206 207
The anticoagulant effect of VKAs such as warfarin can persist for 3–5 days. The need for a rapid correction of VKA-related coagulopathy with reversal agents mainly depends on the severity of haemorrhage, but their use requires caution in patients at high thrombotic risk (eg, mechanical heart valve) since their use has been associated with thromboembolism.208 Vitamin K takes several hours to correct anticoagulation, so the use of 4-factor PCC may be necessary to rapidly reverse anticoagulation in patients with active bleeding and haemodynamic instability. PCC is preferred over FFP, for a lower volume load, faster onset of action, and no need to check the patient’s blood group. Concomitant low-dose vitamin K is recommended in this situation to prevent an ‘INR rebound’.
Unlike VKAs, DOACs are characterised by a relatively short half-lives, so that their anticoagulant activity usually rapidly wanes-off over 12–24 hours. Consequently, most cases of major GI haemorrhage can be managed by withholding the drug and waiting for the anticoagulant effects to resolve. In haemodynamically unstable patients, acute reversal of anticoagulation may be required.209 210 Vitamin K, FFP, and protamine administration are ineffective. Idarucizumab, a humanised antibody fragment that neutralises the effect of dabigatran, is now currently available as first-line reversal agent in dabigatran patients presenting with life-threatening/uncontrolled bleeding.211 212 Idarucizumab reverses dabigatran-related coagulopathy rapidly (within a few minutes) and persistently (for about 24 hours) in more than 98% of the patients, with a low thrombotic complication rate (6% at 90 days). Andexanet alfa, an inactive form of FXa that neutralises circulating FXa inhibitors, has recently been approved as an antidote to apixaban and rivaroxaban in patients with life threatening haemorrhage, but its clinical use is hindered by its limited availability, the prohibitive cost and safety concern about possible procoagulant effect.213 Four-factor PCC at fixed dose (2000 IU) may represent an alternative to andexanet alpha, with lower thromboembolic risk, but uncertain efficacy.214–216
Correction of coagulopathy, when required, should not delay urgent endoscopic or radiological interventions when indicated, as these procedures can be safely and effectively performed at therapeutic levels of anticoagulation in the context of acute haemorrhage.217 218
After bleeding cessation, observational studies219–222 and two meta-analyses223 224 consistently indicate there is a net clinical benefit of restarting anticoagulation, due to a reduced risk of thromboembolism and death, despite an increased risk of rebleeding. However, evidence on the optimal timing for restarting anticoagulation is limited. A single retrospective study indicates an excess risk of GI bleeding and of thromboembolism for an interval of warfarin interruption shorter than 7 days and longer than 30 days, respectively.219 Since there is a trend toward a reduced incidence of thromboembolic events the earlier warfarin is introduced, it is reasonable to restart warfarin as soon as possible by day seven following its interruption. Data on the optimal timing of DOAC resumption are lacking. In analogy with warfarin, restarting DOACs as soon as possible by day seven after their interruption seems reasonable in most cases. The DOAC rapid onset of action, resulting in a full anticoagulation within 2–4 hours, warrants some caution with an earlier resumption.
In patients at very high thrombotic risk (eg, prosthetic metal heart valve in mitral position), cardiology societies recommend an earlier resumption of anticoagulation with UFH in those at highest risk, rapid titration of prophylactic doses of LMWH to therapeutic doses within 48–72 hours.209 210 The choice of strategy should be discussed with the patient’s cardiologist. If the risk of restarting anticoagulation is estimated to outweigh the benefits, a consultation with the referral specialist (haematologist, neurologist and/or cardiologist) is advisable, and alternatives to anticoagulation, such as a left atrial appendage occlusion in AF, or inferior vena cava filter for acute deep venous thrombosis, may be considered.209 210
Ethics statements
Acknowledgments
We gratefully acknowledge the contribution of Dr Sanne Hoogenboom from the Academic Medical Centre, Amsterdam, who undertook the literature searches for risks associated with endoscopic dilatation and endoscopic stenting. We are indebted to Professor Tony Gershlick, an interventional cardiologist who made a major contribution to the antiplatelet advice in the 2008 and 2016 versions of this guideline, and which underpin the recommendations in this update. Professor Gershlick sadly died due to COVID-19 before being able to contribute to this updated document.
References
Footnotes
Twitter @ThrombosisUK
Presented at This article is published simultaneously in the journals Endoscopy and Gut. Copyright 2021 © European Society of Gastrointestinal Endoscopy, all rights reserved and © by BMJ Publishing Group Ltd. This article is published by Thieme Georg Verlag KG, Rüdiger Straße 14, 70469 Stuttgart, Germany.
Contributors AMV convened the guideline development group, assigned tasks, led on recommendations and revisions and edited the final manuscript. All other authors provided written contributions, developed recommendations and provided comments on the complete manuscript prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer These joint BSG and ESGE guidelines represent a consensus of best practice based on the available evidence at the time of preparation. They may not apply in all situations and should be interpreted in the light of specific clinical situations and resource availability. Further controlled clinical studies may be needed to clarify aspects of these statements, and revision may be necessary as new data appear. Clinical consideration may justify a course of action at variance to these recommendations, but we suggest that reasons for this are documented in the medical record. BSG and ESGE guidelines are intended to be an educational device to provide information that may assist endoscopists in providing care to patients. They are not rules and should not be construed as establishing a legal standard of care or as encouraging, advocating, requiring or discouraging any particular treatment.
Competing interests FR has received speaker fees from Bristol-Meyers Squibb, Pfizer and Boehringer Ingelheim. Dr Alikhan has received fees from Alexion, Bayer, Boehringer Ingelheim, Bristol-Meyers Squibb, Daiichi, Pfizer and Portola. WL has received speaker fees from Sanofi Aventis and Leo Pharma, speaker fees and advisory board fees from Bayer, Daichii Sankyo, Pfizer and Boehringer Ingelheim, and support to attend a scientific meeting from Boehringer Ingelheim. JEV-H has received departmental research grant support from Cook Medical and Abbott, lecture fees from Medtronics and Cook Medical, and consultancy fees from Boston Scientific and Olympus.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.