Article Text

Abstract
Objective To determine whether proton pump inhibitors (PPIs) are associated with an increased risk of colorectal cancer, compared with histamine-2 receptor antagonists (H2RAs).
Design The United Kingdom Clinical Practice Research Datalink was used to identify initiators of PPIs and H2RA from 1990 to 2018, with follow-up until 2019. Cox proportional hazards models were fit to estimate marginal HRs and 95% CIs of colorectal cancer. The models were weighted using standardised mortality ratio weights using calendar time-specific propensity scores. Prespecified secondary analyses assessed associations with cumulative duration, cumulative dose and time since treatment initiation. The number needed to harm was calculated at five and 10 years of follow-up.
Results The cohort included 1 293 749 and 292 387 initiators of PPIs and H2RAs, respectively, followed for a median duration of 4.9 years. While the use of PPIs was not associated with an overall increased risk of colorectal cancer (HR: 1.02, 95% CI 0.92 to 1.14), HRs increased with cumulative duration of PPI use (<2 years, HR: 0.93, 95% CI 0.83 to 1.04; 2–4 years, HR: 1.45, 95% CI 1.28 to 1.60; ≥4 years, HR: 1.60, 95% CI 1.42 to 1.80). Similar patterns were observed with cumulative dose and time since treatment initiation. The number needed to harm was 5343 and 792 for five and 10 years of follow-up, respectively.
Conclusion While any use of PPIs was not associated with an increased risk of colorectal cancer compared with H2RAs, prolonged use may be associated with a modest increased risk of this malignancy.
- epidemiology
- colorectal cancer
- acid-related diseases
Data availability statement
No data are available. No additional data available.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Previous observational studies present conflicting evidence regarding the association between proton pump inhibitor use and colorectal cancer incidence.
Previous studies have been limited by small sample sizes, short durations of follow-up, and other methodological shortcomings.
What are the new findings?
The results of this study suggest that any use of proton pump inhibitors is not associated with an increased risk of colorectal cancer.
However, prolonged durations of use of proton pump inhibitors may be associated with a modest increased risk of colorectal cancer.
How might it impact on clinical practice in the foreseeable future?
Given that proton pump inhibitors are commonly overprescribed for inappropriately long durations, this study highlights the need to reassess the need for ongoing treatment regularly.
Introduction
Proton pump inhibitors (PPIs) are commonly prescribed drugs indicated for several gastric conditions, including peptic ulcer disease, GORD and Barrett’s oesophagus.1 2 Histamine-2 receptor antagonists (H2RAs), an alternative class of acid suppressant drugs, are indicated for similar conditions, although they are less effective at lowering stomach acid levels compared with PPIs.1 Recent evidence suggests that PPIs are commonly overprescribed, either in patients without an evidence-based indication for use or longer durations than necessary.3 This is particularly relevant as several observational studies have associated the use of PPIs with different adverse health outcomes, including GI malignancies such as colorectal cancer.4–13
Hypergastrinaemia may be induced by prolonged use of PPIs,14 which in turn, may be associated with the development of colorectal cancer, as hypergastrinaemia has been shown to promote the proliferation of both normal and malignant colonic and rectal cancer cells in vitro.15–20 While animal models suggest that hypergastrinaemia leads to adenoma progression, an important precursor to colorectal cancer,21 the association between PPI use and adenomatous polyps has not been shown consistently in humans.22 To date, several observational studies that investigated the association between PPI use and colorectal cancer have generated conflicting findings (relative risks ranging from 0.85 to 2.54) and had important methodological shortcomings.4–13 Major sources of bias in the existing literature include confounding by indication, the inclusion of prevalent users, and latency bias.23–25 These conclusion-altering biases can lead to spurious and exaggerated associations in both directions, limiting the conclusions drawn from these studies.
Given the conflicting observational evidence, it remains unclear whether the use of PPIs is associated with the incidence of colorectal cancer, a leading cause of cancer death with an increasing incidence among younger adults.26 27 Additional studies are needed to better inform the safety profile of this widely prescribed drug class. Thus, the objective of this large population-based cohort study is to determine whether the use of PPIs, when compared with the use of H2RAs, is associated with an increased risk of colorectal cancer.
Methods
Data source
We used data from the UK Clinical Practice Research Datalink (CPRD), a large, computerised database of longitudinal primary care records of over 15 million patients.28 29 The CPRD contains information on medical diagnoses and procedures, prescription details including dose and quantity, laboratory values and lifestyle characteristics, including smoking and body mass index (BMI). The data have been extensively validated, generating high-positive predictive values and high sensitivities for various diagnoses, including colorectal cancer.30–36 Indeed, the sensitivity, specificity and positive predictive value of colorectal cancer have been estimated at above 90% in several studies.33–35 Moreover, when assessing the validity of 183 different diagnoses, a median of 89% of cases were confirmed using additional internal or external data.36
Study population
We used a new-user, active comparator design to compare patients newly treated with PPIs (including all available in the UK: esomeprazole, lansoprazole, omeprazole, pantoprazole, or rabeprazole; online supplemental table 1) with patients newly treated with H2RAs (including all available in the UK: cimetidine, famotidine, nizatidine, or ranitidine; online supplemental table 2). We selected H2RAs as the comparator group because they represent a clinically relevant group used in similar indications as PPIs and thus should minimise confounding by indication. Cohort entry was defined as the date of this first prescription of either a PPI or H2RA from 1 January 1990, through 30 April 2018. To be included in the cohort, patients were required to be at least 18 years of age and have at least 1 year of medical information in the CPRD before cohort entry; the latter served as a washout period to ensure new use of PPIs and H2RAs. We excluded patients for whom a PPI and an H2RA were prescribed concomitantly at cohort entry and those with a history of Zollinger-Ellison syndrome (a rare indication for PPI use)1 or cystic fibrosis, which is known to increase the risk of early-onset colorectal cancer,37 at any time on or before cohort entry. We also excluded patients with a history of colorectal cancer (ie, to exclude prevalent cases) or rare inherited cancer syndromes (familial adenomatous polyposis, Lynch syndrome, Li Fraumeni syndrome, Peutz-Jeghers syndrome, or Cowden syndrome),38–41 at any time on or before cohort entry. Finally, to allow for a sufficient latency period and minimise detection bias and reverse causality, the cohort was restricted to patients with at least 1 year of follow-up after cohort entry (ie, 1-year lag period).42
Supplemental material
Exposure definition
Patients were considered continuously exposed to their cohort entry drug (ie, first of either PPI or H2RA prescription) starting 1 year after cohort entry until the end of follow-up. This exposure definition, which does not consider treatment termination, aligns with the hypothesised biological mechanism (ie, adenoma progression from prolonged PPI use would progress even following treatment discontinuation). Thus, patients were followed starting 1 year after cohort entry until an incident diagnosis of colorectal cancer (identified using Read codes, online supplemental table 3), 1 year after switching between the study drug classes (ie, switch from PPI to H2RA or vice versa to account for the 1 year lag period, with person-time during the lag period attributed to initial exposure), death from any cause, end of registration with the general practice, or end of the study period (30 April 2019), whichever occurred first. Online supplemental figure 1 illustrates a schematic of this exposure definition.
Potential confounders
We considered the following potential confounders, all measured on or before cohort entry: age (modelled as a continuous variable using a cubic spline model to account for a possible non-linear relation with the outcome),43 sex, alcohol-related disorders, smoking status (current, former, never), BMI, type 2 diabetes, hypertension, coronary artery disease, chronic obstructive pulmonary disease, cancer (other than non-melanoma skin cancer), Crohn’s disease, UC, other IBD, GI polyps, cholecystectomy and solid organ transplant. We also considered the indication for acid suppressant drug use (approved indications: peptic ulcer disease, GORD, dyspepsia, Helicobacter pylori infection, and Barrett’s oesophagus; off-label indications: gastritis/duodenitis and stomach pain). We also included the following drugs previously associated with colorectal cancer incidence, measured at any time before cohort entry: hormone replacement therapy, aspirin, other non-steroidal anti-inflammatory drugs, statins, bisphosphonates, and use of synthetic prostaglandin analogues, which are older drugs used to manage gastric conditions.1 Finally, we included measures of health-seeking behaviours, such as mammographic screening, prostate-specific antigen testing, colorectal cancer screening, and influenza vaccination.
Statistical analysis
We used calendar time-specific propensity scores to reweigh our study population.44 Using multivariable logistic regression, we estimated propensity scores within 5-year calendar bands at cohort entry (1990–1994, 1995–1999, 2000–2004, 2005–2009, 2010–2018) as the predicted probability of receiving a PPI versus an H2RA conditional on the covariates listed above. Calendar time-specific propensity scores were chosen to account for temporal changes in the prescribing of acid suppressants and colorectal cancer incidence during the study period.3 45 Patients in non-overlapping regions of the propensity score distributions were trimmed from the analysis. Using the propensity scores, treatment weights were assigned using standardised mortality ratio weights. Thus, PPI initiators were given a weight of 1, while H2RA initiators were given a weight of the odds of the treatment probability (propensity score/(1-propensity score)).46 This weight functions to upweight the comparator patients (ie, H2RA users) to represent the treated population (ie, PPI users). We assessed covariate balance using standardised differences, with differences of less than 0.10 considered acceptable.47
Incident rates of colorectal cancer, with 95% CIs based on the Poisson distribution, were calculated for each exposure group. Weighted Kaplan-Meier curves were plotted to display the cumulative incidence of colorectal cancer over the follow-up period for PPI and H2RA users. Weighted Cox proportional hazards models were fit to estimate marginal HRs of colorectal cancer with 95% CIs using robust variance estimators. This marginal HR is a population-level estimate that described the average treatment effect in the treated; the average causal effect of treatment in the PPI cohort.46 48 Finally, we calculated the number needed to harm at five and 10 years of follow-up using the Kaplan-Meier method.49
Secondary analyses
We performed five secondary analyses. The first analysis assessed duration–response and dose–response relations according to cumulative duration of use, cumulative omeprazole equivalents, and time since treatment initiation. Cumulative duration was defined by summing the durations of each PPI prescription from cohort entry until the time of the event defining risk set. Given the different potencies of various PPIs, cumulative dose was defined using defined daily doses, a standardised unit of drug consumption defined by the WHO (online supplemental table 4).50 Individual PPI molecules were converted to omeprazole equivalents, and the cumulative dose was calculated by summing the dose of each prescription from cohort entry until the risk set. According to the defined daily dose, a patient prescribed a 30-day course of 30 mg of esomeprazole has equivalent usage to a patient prescribed a 30-day course of 20 mg omeprazole. Finally, time since treatment initiation was defined as the time between cohort entry and the risk set. HRs for these secondary exposures were estimated using time-dependent Cox proportional hazards models using predefined categories (<2 years, 2–4 years and ≥4 years), and cumulative duration and dose were also modelled flexibly using restricted cubic spline models.43 Second, we stratified by type of PPI (omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole or combinations) to determine whether there were any molecule-specific effects. Third, to determine if the association varies by cancer type, we repeated the primary analysis by stratifying on colon versus rectal cancer. Fourth, we considered whether there is effect measure modification by sex, age (<40, 40–59, and ≥60 years), history of IBD (including UC and Crohn’s disease), GI polyps and aspirin use. Age, sex, IBD and GI polyp history are strong nonmodifiable risk factors for colorectal cancer, while aspirin use has been associated with a decreased risk of colorectal cancer.51–56 For these analyses, we included an interaction term in the primary model between exposure status and these variables. Finally, we calculated HRs according to the most common approved indications at baseline (GORD, peptic ulcer disease and dyspepsia).
Sensitivity analyses
We conducted six sensitivity analyses to assess the robustness of our findings. First, we repeated the primary analysis by increasing the exposure lag period to 3, 5 and 10 years, as there are uncertainties regarding the optimal length of the latency window. These analyses were restricted to patients with at least 3, 5 and 10 years of follow-up, respectively. Second, to address the impact of informative censoring, we did not censor patients who switched between drug classes (ie, an intention-to-treat exposure definition). Third, as an alternative method to investigate the impact of informative censoring, we used stabilised inverse probability of censoring weights to account for censoring from switching between drug classes during follow-up,57 58 and to account for the competing risk of death from any cause.59 Censoring weights were calculated using two separate logistic regression models within 1-year intervals, with one estimating the probability of remaining uncensored from a drug switch and the other estimating the probability of not dying (online supplemental method 1). Fourth, as certain H2RAs have recently been found to be contaminated with a probable carcinogen (N-nitrosodimethylamine (NDMA)),60 we repeated the analysis with follow-up truncated on 31 December 2017, which is before the time NDMA contaminants were found.60 Fifth, to investigate the impact of residual confounding, we repeated the analysis using the high-dimensional propensity score (HD-PS) approach to calculate treatment weights (online supplemental method 2).61 For this analysis, we considered all predefined covariates listed above, along with 200 empirically selected covariates from the HD-PS algorithm. Finally, we investigated the potential impact of detection bias from differential screening uptake using inverse probability of screening weighting, estimated within 2-year intervals (online supplemental method 3).62 All analyses were conducted with SAS V.9.4 (SAS Institute) and R V.4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
We did not include patients as study participants as our study involved the use of secondary data. Patients were not involved in the design or implementation of the study. We do not plan to involve patients in the dissemination of results, nor will we disseminate results directly to patients.
Results
The cohort included 1 293 749 and 292 387 initiators of PPIs and H2RAs, respectively (figure 1). Over a median duration of 4.9 years of follow-up (including the 1-year postcohort entry latency period), there were 6759 incident colorectal cancer events among PPI users versus 1264 events among H2RA users. The corresponding crude incidence rates of colorectal cancer were 105.5 (95% CI 103.0 to 108.0) and 87.7 (95% CI 82.9 to 92.7) per 100 000 person years among PPI and H2RA users, respectively.
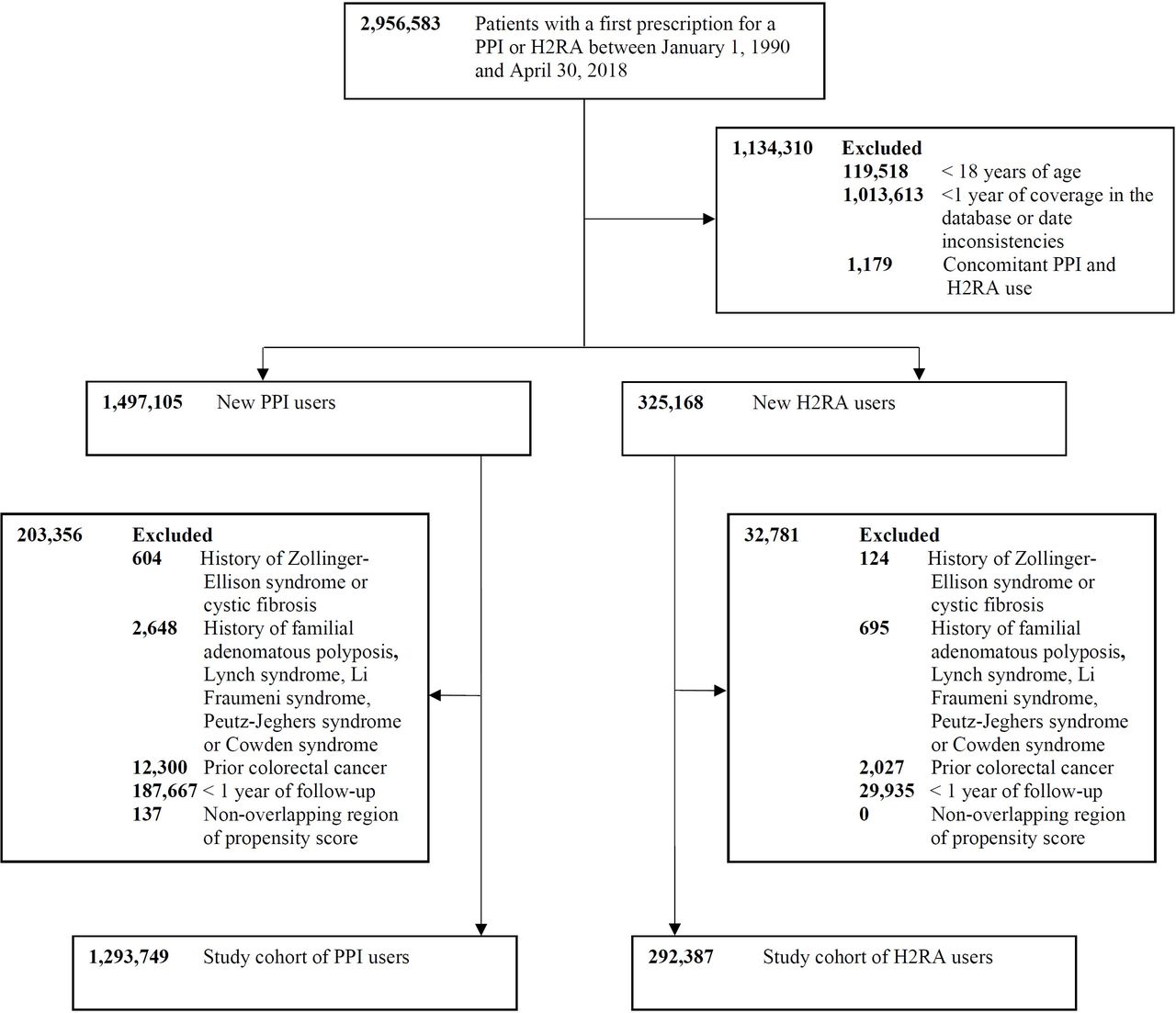
Study flow chart illustrating the construction of the proton pump inhibitor (PPI) and histamine-2 receptor antagonist cohorts (H2RA).
Table 1 shows the baseline characteristics of PPI and H2RA users before and after weighting. Before weighting, the exposure groups were similar in age, sex, history of IBD and cancer. PPI users were more likely to be former smokers, obese, use nonsteroidal anti-inflammatory drugs and statins, and have type 2 diabetes and hypertension, but were less likely to have dyspepsia compared with H2RA users. PPI users were also more likely to be screened for colorectal cancer and have a history of prostate-specific antigen testing. After weighting, the exposure groups were well balanced on all study covariates, with all standardised differences below 0.10. During the follow-up period, 52.8% of H2RA users added-on or switched to PPIs, while 7.7% of PPI users added-on or switched to H2RAs.
Baseline characteristics of proton pump inhibitor and histamine-2 receptor antagonist users before and after weighting
Table 2 shows the results of the primary and secondary analyses. After adjusting for treatment weights, any use of PPIs was not associated with colorectal cancer incidence, compared with the use of H2RAs (HR: 1.02, 95% CI 0.92 to 1.14). The cumulative incidence of colorectal cancer was similar in both exposure groups (online supplemental figure 2). In secondary analyses, there was a gradual increase in risk with increasing cumulative duration of use, cumulative omeprazole equivalents, and time since treatment initiation (table 2). The risk was most elevated in the highest categories of use for all exposure definitions (≥4 years cumulative duration, HR: 1.60, 95% CI 1.42 to 1.80; ≥29 200 mg omeprazole dose equivalents, HR: 1.58, 95% CI 1.39 to 1.78; ≥4 years since treatment initiation, HR: 1.19, 95% CI 1.03 to 1.34) and consistently elevated in the restricted cubic spline models (online supplemental figures 34). The number needed to harm at five years of follow-up was 5343 patients, and at 10 years of follow-up was 792 patients. There was no evidence of molecule-specific effects (online supplemental table 5), and there was no difference in risk when stratifying by colon versus rectal cancer (online supplemental table 6). The association between PPI use and colorectal cancer was modified by sex (male HR: 0.90, 95% CI 0.78 to 1.04; female HR: 1.22, 95% CI 1.04 to 1.45, online supplemental table 7), but was not modified by age, history of IBD, GI polyps or aspirin use (online supplemental tables 8–10). The HR was slightly elevated among patients with dyspepsia at baseline, although the CIs across indications largely overlapped (online supplemental table 12).
Crude and adjusted HRs for the association between the use of proton pump inhibitors and colorectal cancer compared with the use of histamine-2 receptor antagonists
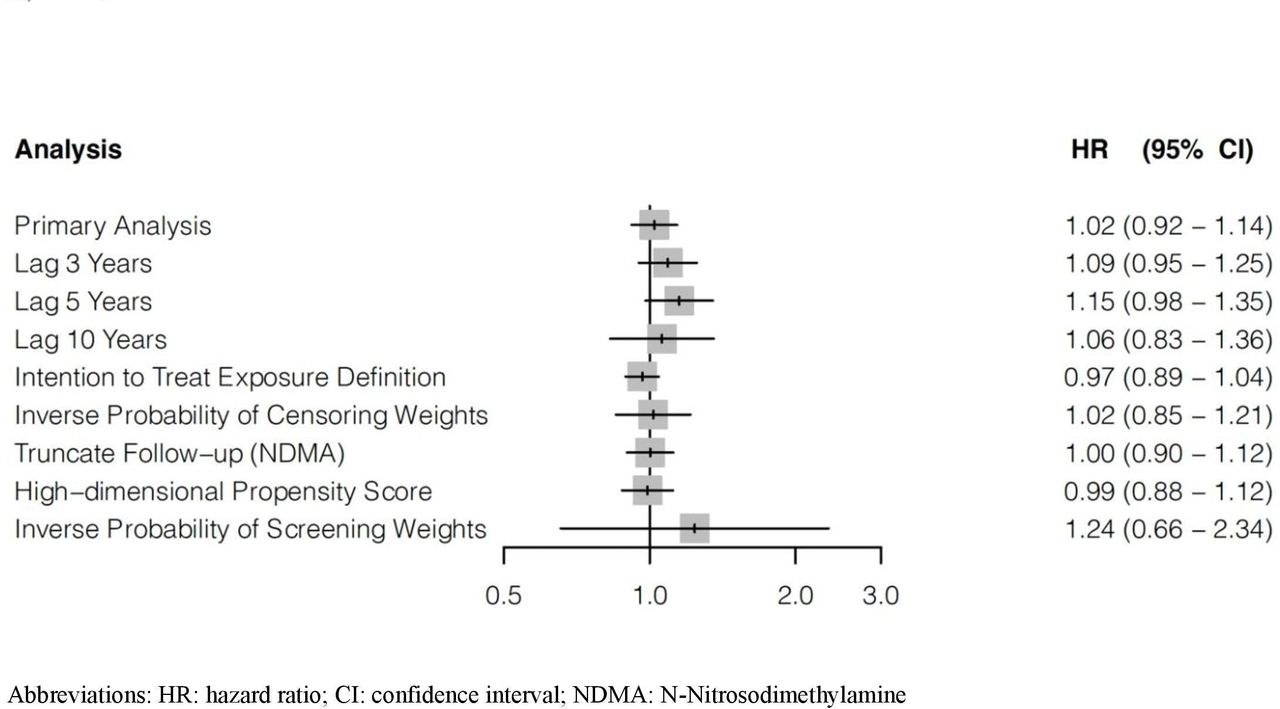
The sensitivity analyses generated highly consistent results (figure 2, online supplemental tables 13 to 18). Overall, the HRs ranged from 0.97 for the intention-to-treat exposure definition to 1.24 for the screening analysis. The screening rate in the PPI and H2RA cohorts was 55.4 and 20.0 per 1000 person years, respectively.

Forest plot summarising the results of the primary and sensitivity analyses, with weighted HRs and 95% CIs for the association between use of proton pump inhibitors and colorectal cancer, compared with the use of histamine-2 receptor antagonists.
Discussion
Principal findings
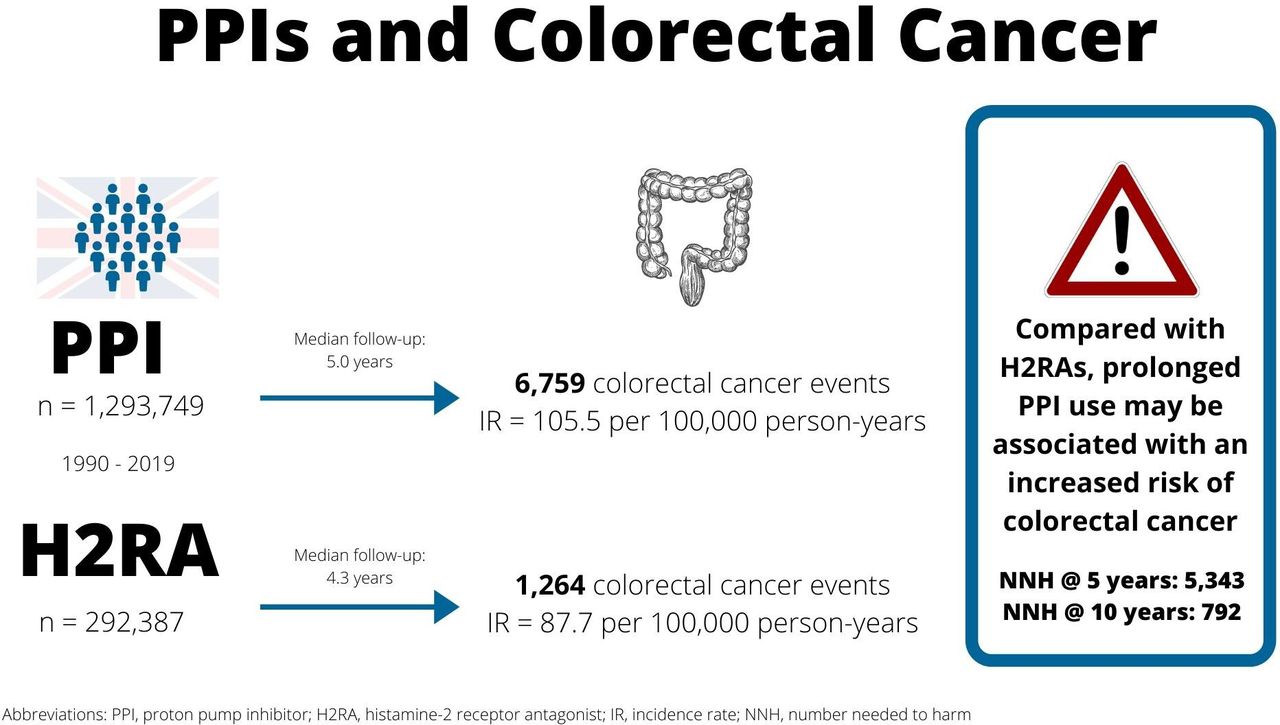
In this large population-based cohort study, we assessed whether initiators of PPIs are at an increased risk of colorectal cancer compared with initiators of H2RAs (figure 3). While any use of PPIs was not associated with an increased risk of colorectal cancer, there was evidence of a duration–response relation, with elevated relative risks with increasing duration, dose and time since initiation. The number needed to harm was 5343 and 792 for five and 10 years of follow-up, respectively. The association was modified by sex, with female PPI initiators at an increased risk of colorectal cancer compared with males. The results remained largely consistent across several sensitivity analyses, although adjustment for screening led to a slight increase in the HR, as colorectal screening is an interventional procedure that decreases the risk of colorectal cancer.63

{kind=link}
{kind=link}
{kind=link}
Graphical summary: graphical summary highlighting the main findings of the association between the use of proton pump inhibitors and colorectal cancer, compared with the use of histamine-2 receptor antagonists.
Comparison with previous studies
The existing evidence on the association between the use of PPIs and overall colorectal cancer risk has been inconsistent, with relative risks ranging from 0.85 to 2.54 (online supplemental table 19).4–13 While the overall results of our study are in line with some of the previous studies,4 5 8–12 few studies found evidence of duration–response relation.5 11 13 However, there are important methodological differences between our study and the previous literature, which may explain some of the discrepant findings. First, while some studies assessed the effect of H2RAs on colorectal cancer risk (relative risks ranging from 0.80 to 2.10),6 7 12 no study used H2RAs as an active comparator. Comparing PPI users to the general population may lead to spurious associations from confounding by indication.23 The previous studies were also limited by other important biases, such as the inclusion of prevalent users, time-related biases like time-window and immortal-time bias, and failure to account for cancer latency.24 25 64 65 In light of these conclusion-altering biases, it is difficult to interpret the existing literature.
The existing biological evidence on the association between PPI use and colorectal cancer is limited. Indeed, chronic suppression of acid through PPI use can induce hypergastrinaemia,14 which has been associated with increased proliferation of normal and malignant colonic and rectal cancer cells in vitro.15–20 However, our findings suggest that for most PPI users who are using PPIs as a short-term treatment, this does not amount to a meaningful increase in the risk of colorectal cancer. Moreover, there is no consensus in the literature as to whether hypergastrinaemia leads to adenoma progression.21 22 While we did not find an increased risk of colorectal cancer from any PPI use, our findings do support the aforementioned biological hypothesis, in that there was a modest increased risk of colorectal cancer among patients prescribed PPIs for increasing durations. Thus, it remains possible that prolonged hypergastrinaemia over an extended period may lead to increased colorectal cancer risk among long-term PPI users. This association may also be explained by changes to the gut microbiome induced through PPI use,66 67 which can alter colorectal cancer susceptibility and progression.68
Strengths and limitations of this study
This study has several strengths. First, to our knowledge, this is the largest study with the longest potential follow-up conducted to date. Second, contrary to previous studies, we used an active comparator for our analyses, minimising confounding by indication and presenting a clinically meaningful comparison. Third, our new-user study design eliminated the biases associated with the inclusion of prevalent users, such as survival bias and confounding. This active comparator new-user study design also minimises the possibility of immortal time bias, as person time at risk starts after the initiation of treatment.69 Fourth, we used propensity score-weighted models, which ensured that baseline confounders were well balanced between our study groups. Finally, we present measures of absolute risk, which are important in understanding the potential burden of colorectal cancer in patients using PPIs.
This study has certain limitations that need to be considered. First, there may be some exposure misclassification, as the CPRD captures prescriptions issued by general practitioners and does not contain data on specialist prescriptions or over-the-counter use. However, in the UK, general practitioners are responsible for the long-term care of gastric disorders,70 and patients with underlying disease, for whom moderate-to-long-term treatment is indicated, are financially incentivised to receive prescriptions from their general practitioner rather than from over-the-counter. Nonetheless, we expect any potential exposure misclassification to be non-differential between the exposure groups. It was also not possible to measure treatment adherence, although this is unlikely to be differential between the exposure groups. Second, we were unable to stratify the outcome according to cancer stage or tumour site (colon vs rectal or left-sided vs right-sided colon), as these variables are not available in the CPRD. This would have been useful to understand whether any observed increased risk of colorectal cancer was a result of increased detection. Third, the prevalence of screening may be underestimated in this cohort.71 Finally, as with all observational studies, residual confounding from unknown or unmeasured confounders is possible, including family history, diet, or ethnicity. We attempted to minimise the impact of residual confounding using an active comparator and a wide variety of potential confounders in our propensity score models. Moreover, the results from the HD-PS analysis, which included an additional 200 covariates, which may be proxies for unknown or unmeasured confounders,61 generated highly consistent findings.
In summary, the results of this study suggest that while any use of PPIs is not associated with an increased risk of colorectal cancer compared with the use of H2RAs, prolonged use might be associated with an increased risk of this malignancy. Though the absolute risk of colorectal cancer is low at the individual level, given the high prevalence of PPI use, this increased risk could translate to a significant excess number of colorectal cancer cases at the population level. In light of this risk, PPIs should be deprescribed in patients for whom treatment is no longer indicated, and physicians should closely monitor patients that require long-term PPI treatment.
Data availability statement
No data are available. No additional data available.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the Independent Scientific Advisory Committee of the CPRD (protocol number 21_000341) and by the Research Ethics Board of the Jewish General Hospital.
Acknowledgments
This study was funded by a Foundation Scheme Grant from the Canadian Institutes of Health Research (FDN-143328). The sponsor had no influence on the design and conduct of the study, collection, management, analysis, or interpretation of the data, and preparation, review, or approval of the manuscript. DA is the recipient of a Vanier Canada Graduate Scholarship from the Canadian Institutes of Health Research. EGM holds a Chercheur-Boursier award from the Fonds de Recherche du Québec – Santé. MES holds a Canadian Institutes of Health Research Canada Research Chair, Tier 2. SS is the recipient of the Distinguished James McGill Professorship award. LA holds a Chercheur-Boursier Senior award from the Fonds de Recherche du Québec – Santé and is the recipient of a William Dawson Scholar Award from McGill University.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors conceived and designed the study. LA acquired the data. DA and LA did the statistical analyses. MES and SS provided statistical expertise. All authors analysed and interpreted the data. EGM and ANB provided clinical expertise. DA wrote the manuscript, and all authors critically revised the manuscript. LA supervised the study and is the guarantor. All authors approved the final version of the manuscript and agree to be accountable for the accuracy of the work.
Competing interests SS participated in advisory meetings or as a guest speaker for Atara Biotherapeutics, Boehringer-Ingelheim, Bristol-Myers-Squibb, Merck and Pfizer, all unrelated to this study. LA served as a consultant for Janssen and Pfizer for work unrelated to this study. The other authors have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.