Article Text

Abstract
Background and aim Mesenchymal stromal cells (MSCs) are pluripotent cells that have immunosuppressive effects both in vitro and in experimental colitis. Promising results of MSC therapy have been obtained in patients with severe graft versus host disease of the gut. Our objective was to determine the safety and feasibility of autologous bone marrow derived MSC therapy in patients with refractory Crohn's disease.
Patients and intervention 10 adult patients with refractory Crohn's disease (eight females and two males) underwent bone marrow aspiration under local anaesthesia. Bone marrow MSCs were isolated and expanded ex vivo. MSCs were tested for phenotype and functionality in vitro. 9 patients received two doses of 1–2×106 cells/kg body weight, intravenously, 7 days apart. During follow-up, possible side effects and changes in patients' Crohn's disease activity index (CDAI) scores were monitored. Colonoscopies were performed at weeks 0 and 6, and mucosal inflammation was assessed by using the Crohn's disease endoscopic index of severity.
Results MSCs isolated from patients with Crohn's disease showed similar morphology, phenotype and growth potential compared to MSCs from healthy donors. Importantly, immunomodulatory capacity was intact, as Crohn's disease MSCs significantly reduced peripheral blood mononuclear cell proliferation in vitro. MSC infusion was without side effects, besides a mild allergic reaction probably due to the cryopreservant DMSO in one patient. Baseline median CDAI was 326 (224–378). Three patients showed clinical response (CDAI decrease ≥70 from baseline) 6 weeks post-treatment; conversely three patients required surgery due to disease worsening.
Conclusions Administration of autologous bone marrow derived MSCs appears safe and feasible in the treatment of refractory Crohn's disease. No serious adverse events were detected during bone marrow harvesting and administration.
- Crohn's Disease
- mesenchymal stem Cell
- mesenchymal stromal Cell
- MSC
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
MSCs have immunosuppressive effects on T and B cells.
MSCs ameliorate experimental colitis.
MSCs are effective in the treatment of acute and severe GvHD of the gut.
What are the new findings?
MSCs derived from the bone marrow of refractory Crohn's disease patients have identical characteristics compared to MSCs from healthy donors and have intact immunomodulatory capacities in vitro.
Administration of autologous bone marrow-derived MSCs is safe and feasible in the treatment of refractory Crohn's disease.
How might it impact on clinical practice in the foreseeable future?
In this manuscript we describe the results of a phase I trial on the application of MSCs in luminal Crohn's disease. Our observations can be the basis for further clinical trials on autologous bmMSCs as a potential treatment for Crohn's disease.
Introduction
Inflammatory bowel diseases are chronic inflammatory disorders of the gastrointestinal tract, including Crohn's disease and ulcerative colitis. Despite the improvements in the management of inflammatory bowel diseases with the introduction of anti-tumour necrosis factor (TNF) compounds, remission often remains difficult to maintain. Many patients suffer from a poor quality of life due to disease relapse, repeated surgeries, extra-intestinal manifestations and drug side-effects. Therefore, novel therapeutic approaches need to be explored.
Mesenchymal stromal cells (MSCs) are non-haematopoietic stromal cells exhibiting multi-lineage differentiation capacity and the ability to mediate immunosuppressive and anti-inflammatory effects.1–3 MSCs are easily isolated from various tissues,4–6 including the bone marrow, and are capable of ex vivo expansion. Moreover, MSCs can be cryopreserved without loss of phenotype or differentiation potential.7 Systemic infusion of MSCs ameliorated the clinical and histopathological severity of experimental colitis, abrogating body weight loss, diarrhoea, and inflammation and increasing survival.8 9 Furthermore, in humans, transplantation of bone marrow (bm) derived MSCs has led to improvement of corticoid refractory graft versus host disease (GvHD), including GvHD of the gut10 11 and MSCs obtained from adipose tissue induced healing in complex perianal fistulas in patients with Crohn's disease.12 Although the mechanisms underlying these effects are not fully elucidated, it has been shown that both cell–cell contact and the secretion of growth factors and cytokines are involved.13 14 The potential role of MSCs in the modulation of immune responses and tissue regeneration aroused interest to use MSCs as a novel cellular therapy to treat Crohn's disease.15
In this clinical phase I study, we evaluated the safety and feasibility of intravenous infusion of autologous bmMSC in refractory Crohn's disease patients. Additionally, the functionality of these bmMSCs was studied focussing on culture potential, morphology, cell surface marker profiling, differentiation potential and immunosuppressive properties. Finally, the effect of bmMSCs on various drugs used to treat Crohn's disease was assessed.
Methods
Patient selection
On 14 January 2008, the Medical Ethical Committee of the Leiden University Medical Center (LUMC) and the Central Committee on Research involving Human Subject (CCMO, The Hague, the Netherlands) approved this phase I study on autologous bmMSCs in the treatment of refractory Crohn's disease (registered in the Netherlands National Trial Register under study number NTR1360 http://www.trialregister.nl/). All patients gave written informed consent. Criteria for patient inclusion were that patients were at least 18 years of age and had moderate to severe Crohn's disease, as defined by a baseline Crohn's Disease Activity Index (CDAI) score between 220 and 450. Furthermore, patients had to be refractory to the standard treatment options for Crohn's disease. We defined refractory patients as patients that, at some time during the course of the disease, must have received steroids, immunosuppressive agents (eg, azathioprine, 6-mercaptopurine or methotrexate) or anti-TNF therapy which did not result in an adequate response to treatment. The following medications were allowed: 5-aminosalicylates and corticosteroids (at a stable dosage regimen for at least 4 weeks) and methotrexate, azathioprine or 6-mercaptopurine (at least 12 weeks, with stable dosage regimen for at least 8 weeks). Infliximab was discontinued at least 8 weeks prior to enrolment. All patients continued current treatment at the time of infusion. Before bone marrow harvest for MSC isolation and expansion, patients were thoroughly screened including medical history, physical examination, standard laboratory investigations and chest x-ray to rule out tuberculosis. Each patient was also screened for HIV, syphilus, hepatitis B and C virus. Patients were excluded if they had a history of lymphoproliferative disease or malignancy within the past 5 years, when they exhibited serious infections or when in need of immediate surgery. Colonoscopy was performed at baseline to confirm disease activity.
Laboratory methods for clinical expansion of MSCs
MSC isolation and expansion
MSCs were expanded according to a common protocol devised by the European Group for Blood and Bone Marrow Transplantation developmental committee, as previously described.10 Bone marrow was harvested by aspiration from the iliac crest from patients under local anaesthesia in the outpatient clinic. Bone marrow mononuclear cells (MNCs) were isolated by Ficoll density gradient (density 1.077 g/cm3) centrifugation. Washed cells were resuspended in Dulbecco's modified Eagle's-low glucose medium (Invitrogen, Paisley, UK) supplemented with penicillin and streptomycin (Lonza, Verviers, Belgium) and 10% fetal bovine serum (FBS; HyClone, Logan, Utah, USA), without any additional growth factors. MNCs were plated at a density of 160 000 cells/cm2. Cultures were maintained at 37°C in a humidified atmosphere containing 5% CO2 in 175 cm2 flasks (Greiner Bio-One, Frickenhausen, Germany). When the cultures reached near confluence (>80%), the cells were detached by treatment with trypsin/EDTA (Lonza, Verviers, Belgium) and replated at a density of 4000 cells/cm2. MSCs were passaged up to a maximum of three times. When sufficient MSCs were expanded, cells were harvested and cryopreserved in isotonic buffered salt solution supplemented with 10% dimethyl sulfoxide (LUMC Pharmacy, Leiden, The Netherlands). Data on MSCs obtained from healthy donors matched for age and gender, was obtained from previous studies.10 16 17 MSCs for these studies were sourced either from a family or non-related (third party) donor. Donors were informed about and consented to the possibility of the use of their MSCs for preclinical studies/analysis. All donors underwent routine donor control examination and screening tests, according to the standard procedures required for bone marrow donors. Following eligibility, donors donated 50–100cc of bone marrow under local anaesthesia as described above.
Characterisation of MSC products
Morphology was monitored twice a week throughout the culture period by light microscopy. Cell viability was determined at each passage and harvest procedure by Trypan blue staining in a Bürker chamber. Immunophenotyping of cultured MSCs was performed using flow cytometry. The following markers were analysed: HLA II (DR), CD73, CD90, CD31, CD34, CD45, CD80 (Becton Dickinson, Franklin Lakes, New Jersey, USA) and CD105 (Ancell, Bayport, Minnesota, USA). The samples were analysed on a FACSCalibur using CellQuest Pro software (Becton Dickinson). Absence of contamination by pathogens was tested at culture initiation and harvest of the MSC product by aerobic and anaerobic cultures (Bactec plus aerobe/F and Bactec plus anaerobe/F; Becton Dickinson). Genetic stability of the expanded MSCs was tested by karyotype analysis using a standard G-banding procedure.
Clinical application of MSC products
Release criteria for clinical use of MSCs included product sterility, absence of visible cell clumps, spindle-shape morphology, expression of CD73, CD90 and CD105 surface molecules (>90%) and a normal karyotype in at least 20 observed metaphases.
Laboratory methods for supportive research
In vitro differentiation
MSCs were plated at 5×104 cells/cm2 in 24-well culture plates and kept in complete medium until 80–90% confluency was reached. For osteogenic differentiation cells were stimulated for 21 days in standard medium supplemented with 50 μg/ml ascorbic acid, 10 mM β-glycerolphosphate and 10−8 M dexamethasone and were stained with fast blue for alkaline phosphatase. For adipogenic differentiation, cultures were stimulated for 21 days with complete medium supplemented with 0.5 mM 3-isobutyl-1-methylxanthine, 100 μM indomethacin, 5 μg/ml insulin and 10−6 M dexamethasone. Lipid droplets were revealed by staining with Oil Red O. Control MSCs were grown in non-conditioned medium. All chemicals were from Sigma-Aldrich (St Louis, Missouri, USA).
MSC/peripheral blood mononuclear cell proliferation assay
Cultured MSCs from patients with Crohn's disease were plated in flat-bottom 96-well plates (Costar, Zwijndrecht, the Netherlands) and allowed to attach overnight. PBMCs were isolated from whole blood of patients with Crohn's disease before MSC infusion. PBMCs were stimulated anti-CD28/anti-CD3 coated Dynabeads (1 bead/5 cells; Invitrogen) per 1×106 cells and were seeded in IMDM with 5% human serum (Sanquin, Amsterdam, The Netherlands), 5% FBS and 100 IU/ml IL-2 (LUMC Pharmacy) per well. Proliferation was measured by 3H-thymidine incorporation. In order to test the effect of MSCs in addition to Crohn's disease medication on proliferationg PBMCs, the proliferation assay was also performed in the presence of indicated medications: 10 μg/ml infliximab, 10 μg/ml adalimumab, 10 μM dexamethasone (Sigma-Aldrich), 1 μM azathioprine (Sigma-Aldrich), 4 μm 6-mercaptopurine (Sigma-Aldrich), and 100 μg/ml methotrexate (Pharmachemie BV, Haarlem, The Netherlands) performed as described above.
Cell bead array cytometric assay
Production of TNFα, interleukin (IL)-1b, IL-10, and IL-6 in MSC/PBMC supernatants, colon biopsy homogenates and serum was determined using a CBA kit according to the manufacturer's instructions (BD Biosciences, San Jose, CA).
Study design
Patients received two doses of MSCs, 7 days apart, at weeks 0 and 1. Just before clinical application, cryopreserved cells were thawed and cells were infused intravenously at a target dose of 1–2×106 cells/kg body weight. Patients were clinically assessed at weeks 0, 1, 2, 4, 6 and 14. At each visit, adverse events were ascertained, concomitant medications were recorded and samples for clinical laboratory evaluations and the patients' CDAI scores were obtained. Colonoscopies were performed at weeks 0 and 6, and mucosal inflammation was assessed using the Crohn's disease endoscopic index of severity (CDEIS). The study flow chart is depicted in figure 1.

Study flow chart.
Statistical analysis
Data were analysed using SPSS or GraphPad. Analyses included the Kruskall–Wallis test followed by Dunn's multiple comparisons (multiple comparisons), two-sided t test and the Wilcoxon signed-rank test for paired data. p Values <0.05 were considered significant.
Results
Patients
In total ten patients (eight females/two males, median age 32.5 and range 19–42 years) with moderate to severe Crohn's disease (median CDAI score at screening of 299.5 and range 255–442) were included in the study and underwent bone marrow aspiration under local anaesthesia. Besides some local pain at the puncture site afterwards, bone marrow aspiration was well tolerated by all patients. Baseline characteristics are presented in table 1. The bone marrow aspiration procedure resulted in sufficient bone marrow to expand MSC up to the required therapeutic doses (supplementary table 1).
Baseline characteristics of included patients
One patient with a CDAI score of 255 at screening showed no active disease on colonoscopy and was therefore excluded for further MSC administration (patient 9). The baseline median CDAI score of the nine treated patients was 326 (range 224–378). During MSC infusion, patients were closely monitored. MSC infusion was successful and without relevant side effects. In one patient a transient mild allergic reaction occurred which was probably due to the cryopreservant DMSO. Moreover, all patients noticed the typical smell and taste due to the DMSO up to 48 h after infusion. Other adverse events in the first 6 weeks of the protocol were ruled unlikely to be associated with MSC treatment and included adverse events such as common cold and headache (table 2).
Adverse events in MSC treated patients (weeks 0–6)
bmMSC from refractory Crohn's disease patients are comparable to MSCs from healthy donors
Approximately 100 ml of bone marrow was aspirated from each patient and bmMSCs were isolated and cultured. MSCs from Crohn's disease patients showed the typical spindle-shaped morphology and similar growth potential and yield compared to MSCs from healthy donors (Supplementary figure 1). Depending on the number of cells needed and the yield of cells, MSCs were harvested in the first, second or third passage (Supplementary table 1). All MSC cultures showed normal karyotyping. Immunophenotypical characterisation was performed by FACS analysis, and showed similar phenotyping as described for healthy controls (table 3).
Flow cytometric analysis of cultured bone marrow mesenchymal stromal cells from patients with Crohn's disease and healthy donors matched for gender and age (mean/median age of patients with Crohn's disease patients 31.3/32.5 and healthy donors 32.1/32.5)
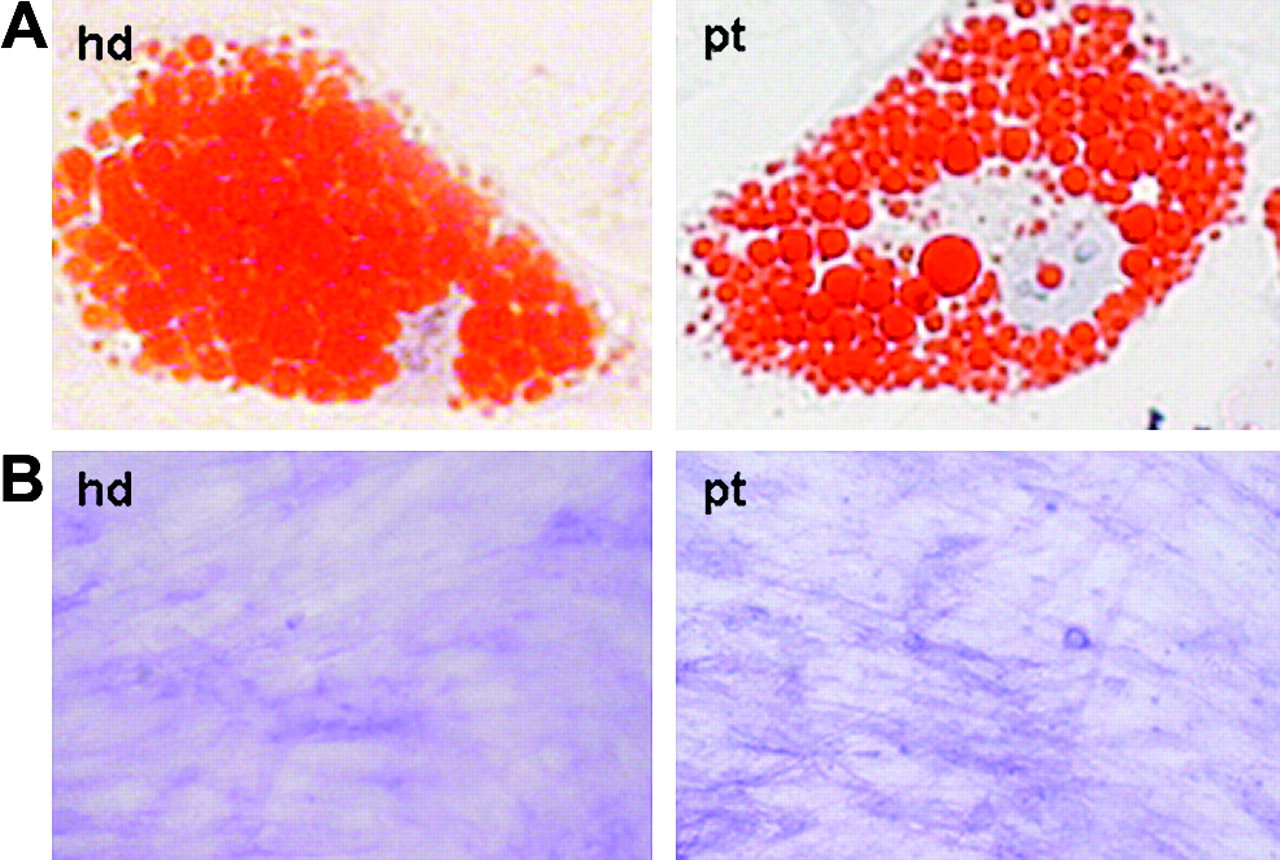
Furthermore, Crohn's disease MSCs were able to differentiate along the osteogenic and adipogenic lineages when cultured in appropriate culture medium (figure 2).

Mesenchymal stromal cells (MSCs) from Crohn's disease patients differentiate into mesenchymal lineages. (A) Adipocyte differentiation was demonstrated in MSCs cultured from a healthy donor (hd) and from a patient with Crohn's disease (pt) after which cells were stained with Oil Red O to show lipid droplets in the cytoplasm of the cell. (B) For osteoblast differentation MSCs were stained with fast blue to show alkaline phosphatase activity. Non-conditioned MSCs did not stain for Oil Red O, whereas fast blue gave slight background staining (not shown).
bmMSCs from refractory Crohn's disease patients suppress immune responses in vitro
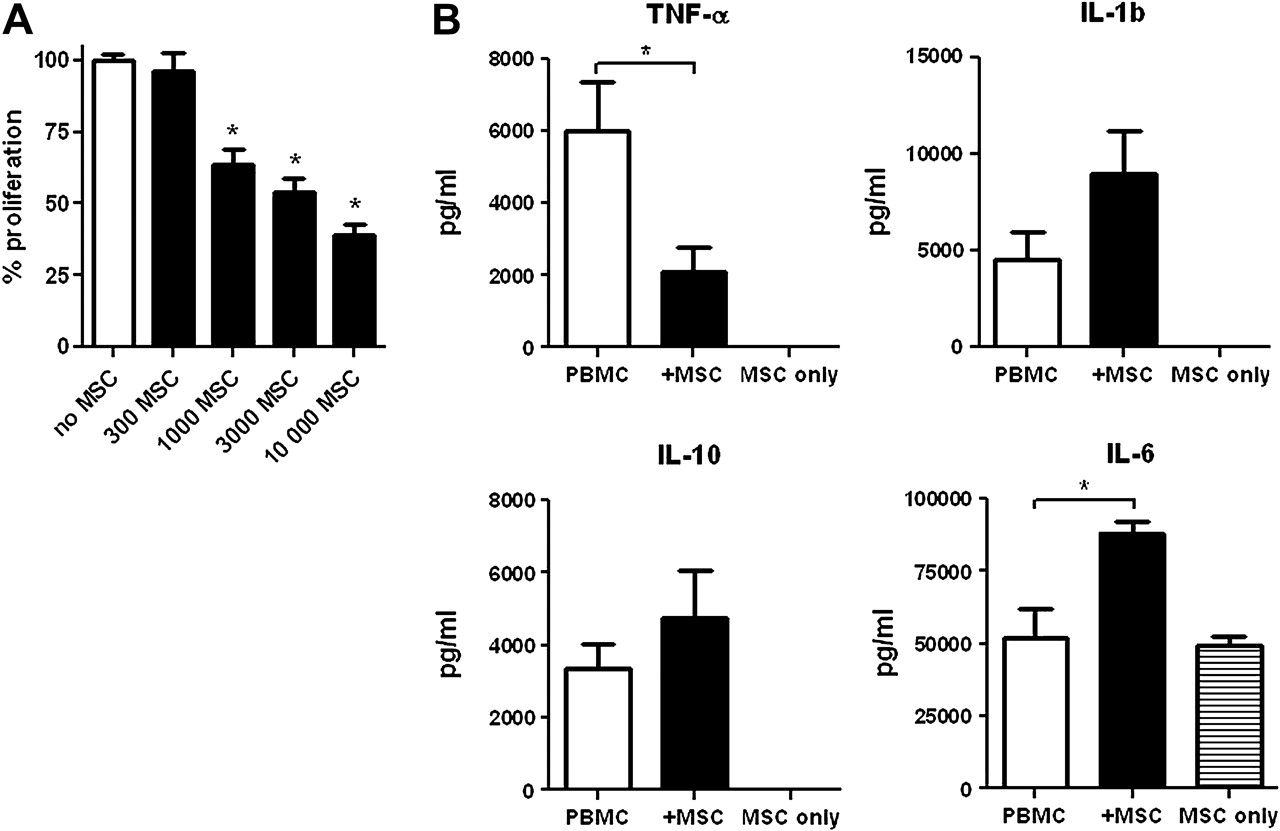
In the presence of autologous bmMSCs proliferation of PBMCs was reduced in a cell dose-dependent fashion (figure 3A) and decreased TNFα production was observed. An increase of IL-1b and IL-6 was seen, as well as an increase in the regulatory cytokine IL-10 (figure 3B). MSC proliferation was not affected by co-medication (infliximab, adalimumab, dexamethasone, azathioprine, 6-mercaptopurine and methotrexate) in vitro (data not shown). However, MSCs do have an additive effect on inhibition of PBMC proliferation by various Crohn's disease medication in vitro (figure 4).

Mesenchymal stromal cells (MSCs) from Crohn's disease patients significantly inhibit the proliferation of autologous peripheral blood mononuclear cells (PBMCs) and this inhibition is dose-dependent. (A) 100 000 PBMCs were stimulated with anti-CD3/CD28 beads in the absence (white column) or presence (black columns) of indicated numbers of autologous MSCs. Proliferation measured by 3H-thymidine uptake in counts per minute was expressed as a percentage of PBMC proliferation without MSCs for each individual patient. (B) Cytokine production in the supernatants of PBMC cultures and 10 000 MSC/100 000 PBMC co-cultures. MSCs alone produce interleukin 6 (IL-6) (lower right). In the presence of MSCs, tumour necrosis factor α (TNF-α) production is lowered, whereas IL-1b, IL-6 and IL-10 production is increased. Bars represent the mean and SEM of data from 10 patients in triplicate. *p<0.05 for significant differences.

Mesenchymal stromal cells (MSCs) have an additive effect on the inhibition of peripheral blood mononuclear cell (PBMC) proliferation by Crohn's disease medication. In the presence of indicated Crohn's disease medication proliferation of 100 000 stimulated PBMCs added to 1000 MSCs (black bars) compared to PBMC without MSCs (white bars) was measured. Proliferation measured by 3H-thymidine uptake in counts per minute was expressed as a percentage relative to PBMC proliferation in control medium (set to 100%). Bars represent mean and SEM. *p<0.05 for significant differences between test conditions based (two-sided t test). ADA, adalimumab; AZA, azathioprine; DEX, dexamethasone; IFX, infliximab; 6-MP, 6-mercaptopurine; MTX, methotrexate.
Clinical response
Clinical assessment was performed on all patients using CDAI scoring. Two patients were excluded before the primary endpoint was met. The first patient was a chronic severe steroid refractory patient on the waiting list for surgery. Although an initial decrease of CDAI score was seen this patient was excluded when presented with a CDAI >450 due to poor general condition and persistent rectal blood loss. Patient 7 was withdrawn from the study 4 days after the first MSC infusion because of continuing abdominal aches and bloody diarrhoea. In this case infliximab treatment was resumed. CDAI scores improved in five patients, clinical response (defined as a drop in CDAI >70) was seen in three patients at week 6 (table 4).
Clinical scores of patients at week 0, 1 and 6. In the 6 month follow-up period, three patients underwent surgery in the indicated week after mesenchymal stromal cell infusion
Remission (CDAI <150) was not achieved in any of the patients. Three patients had a reduction of 70 points in CDAI score, this decrease could in most cases be ascribed to solid stools and a decrease in soft stool frequency. In a period of 14 weeks, three patients required surgery due to disease worsening (table 4). No significant differences in C-reactive protein (CRP) levels were seen.
Endoscopy
Endoscopic improvement, observed by a decrease in CDEIS of 10.0 and 24.7 points, was seen in two patients with extensive Crohn's disease localised in the colon (figure 5). In the other five patients no significant endoscopic improvement was seen between baseline and 6 weeks post-infusion. At weeks 0 and 6, levels of CD4+, CD8+ and CD4+CD127+ populations were determined in biopsies of inflamed mucosa (figure 6A left panels). A trend of lower CD4+ T cells and higher CD4+CD127+ regulatory T cells were observed at week 6 when compared to week 0. Cytokine levels of TNFα, IL-1b, IL-10 and IL-6 were determined in mucosal biopsies and serum at weeks 0 and 6. In general, cytokine levels decreased in the mucosa (figure 6A right panels), whereas an increase of cytokine levels in the serum was seen (figure 6B).

Endoscopy at week 0 (upper panels) and at 6 weeks (lower panels) after mesenchymal stromal cell (MSC) treatment (two administrations of 2×106 autologous bmMSCs) shows clear mucosal healing. Pictures A and B are from patient 2, pictures C and D from patient 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CD4+, CD8+ and CD4+CD127+ populations in biopsies of inflamed mucosa at weeks 0 and 6 (A, left panels). Cytokine levels of tumour necrosis factor α (TNFα), interleukin-1b (IL-1b), IL-10 and IL-6 were determined in mucosal biopsies (A, right panels) and serum (B) at weeks 0 and 6. Bars represent mean and SEM. *p<0.05 for significant differences.
Discussion
This phase I study shows that bone marrow harvesting and expansion of bmMSCs from patients with refractory Crohn's disease is feasible and that MSCs cultured from patients with Crohn's disease are similar to MSCs from healthy donors, in plastic adherence, spindle-shaped morphology, growth potential (supplementary figure 1), surface marker expression, lack of haematopoietic markers (table 3) and differentiation capability (figure 2). In addition, MSCs from refractory Crohn's disease patients are able to inhibit autologous PBMC proliferation and inhibit TNFα production in vitro (figure 3). Furthermore, autologous bmMSC infusion appears to be safe as intravenous MSC infusions were clinically well tolerated. Reported adverse events directly related to MSC infusion were a mild and transient allergic reaction in one patient and the typical taste and smell of the cryopreservant DMSO noticed by all patients (table 2).
Although the design of this study does not allow conclusions on efficacy, after two infusions with autologous bmMSCs, endoscopic improvement was seen in two patients (figure 5), while three patients required surgery due to worsening of disease (table 4). Patients included were chronic active patients refractory to all currently available medical therapeutic options. One could speculate that the immunomodulatory effect of MSCs might not be sufficient to induce clinical remission in this category of patients. Further (randomised) trials in also less refractory patients are therefore warranted
In order to study the biologial effects of systemic MSC infusion in patients with refractory Crohn's disease we analysed CD4+CD127+ expression on T cells obtained from colonic biopsies and determined cytokine production in both colon homogenates and serum. We observed a trend of lower CD4+ T cells and higher CD4+CD127+ regulatory T cells at week 6 when compared to week 0, although the number of patients in this study was not enough to reach statistical significance. In addition, cytokine levels went down in mucosal biopsies, indicating a decrease in intestinal inflammation (figure 6A right panels). The apparent reciprocal increase in serum cytokine levels (figure 6B) may be the result of altered distribution of inflammatory cells. Due to the decreased local inflammation, leucocytes are no longer recruited to the intestine, but remain in the circulation, thus increasing the systemic cytokine levels. Similar findings have been observed for regulatory T cells in Crohn's disease18 and plasmacytoid dendritic cells in dermal inflammation.19
The intravenous route of administration and target dose of 1–2×106 cells/kg body weight were based on experience with other protocols in GvHD. Intravenous infusion of cells is an easy, minimal invasive and routinely performed procedure with proven safety so far. Although it has been suggested that MSCs home to sites of inflammation, it is unknown how many cells will eventually reach the intestine in patients with Crohn's disease. In a case report, Dinesen et al20 showed that administration of MSCs via selective mesenteric artery cannulation was safe and feasible. This approach may possibly increase the number of cells reaching the affected organ.
In the case of autologous MSCs, an ongoing discussion is whether MSCs are affected by or may contribute to the underlying disease. For instance, MSCs from patients with systemic lupus erythematosus are difficult to expand in culture and yield low cell numbers21 and those from patients with multiple myeloma have been shown to be impaired and possibly contribute to the pathogenesis of the disease.22 In this study we demonstrate that MSCs obtained from patients with refractory Crohn's disease show similar growth potential, yield and properties when studied in vitro in comparison to MSCs from healthy donors. Our data support work published recently23 and suggest that bmMSCs from patients with refractory Crohn's disease are not affected by the disease. Unfortunately, there is no ‘gold standard’ test to assess the functionality of MSCs and it has not been demonstrated that in vitro effectiveness of MSCs can be translated to clinical effectiveness, making true extrapolation of this topic difficult.
Another important issue is the effect of MSCs on concomitant medication.24 To address this matter, we studied the effect of MSCs on various routinely used Crohn's disease medications in vitro. We found that adding various Crohn's disease medications to MSC cultures did not affect cell proliferation. Furthermore, adding MSCs to proliferating PBMCs in the presence of tested medications, gave a cumulative effect on the inhibition of PBMC proliferation (figure 4), suggesting that MSCs can be used in addition to concomitant Crohn's disease medication.
A concern in cell-based therapies with ex vivo expanded cells is the formation of tumours. Previous work indicated that, in mice, MSCs stimulate the growth of cancers25 26 and promote metastasis.27 Additionally, extensive in vitro expansion of cells may induce genetic instability. Although an increased risk on tumour formation has never been confirmed in humans, patients with a history of malignancy were excluded from this study. To minimise the risk of transformation of cells we have expanded MSCs in the absence of growth factors, plated MSCs in moderate cell concentrations and used only low passage numbers. Furthermore, we karyotype the MSC product before clinical release to confirm normal karyotyping and did not observe any aberrancies.
In conclusion, our data suggest that intravenous application of autologous bmMSCs is feasible and well tolerated. Furthermore, bmMSC administration may produce clinical benefits in severe refractory Crohn's disease. Therefore, further studies should be designed to examine MSCs as a potential treatment for Crohn's disease.
Acknowledgments
We would like to thank Akin Inderson and Stefanie Kraus for performing bone marrow punctions, Marthe Verwey and Maartje Holsbergen-De Ley for collecting patient data and the technicians of the stem cell laboratory of the LUMC for MSC expansion.
References
Supplementary materials
Web Only Data gut.2010.215152
Files in this Data Supplement:
{kind=link}
Footnotes
Funding This work was supported by grants from the Dutch Digestive Diseases Foundation (MLDS, W07-17), Digest Science Grant and a grant from ZonMW (TAS).
Competing interests None declared.
Ethics approval This study was conducted with the approval of the Medical Ethical Committee of the Leiden University Medical Center (LUMC) and the Central Committee on Research involving Human Subjects (CCMO, The Hague, The Netherlands). http://www.trialregister.nl/ identifier: NTR1360.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest