Article Text

Abstract
BACKGROUND/AIM The effects of different prokinetic agents, the motilide erythromycin and the substituted benzamides metoclopramide and cisapride, were investigated in a rat model of postoperative ileus. These effects were compared with that of granisetron, a 5-hydroxytryptamine (5-HT3) receptor antagonist, and a novel enterokinetic agent, prucalopride, a 5-HT4 receptor agonist.
METHODS Different degrees of inhibition of gastrointestinal transit, measured by the migration of Evans blue, were achieved by skin incision, laparotomy, or laparotomy plus mechanical stimulation of the gut.
RESULTS Metoclopramide decreased the transit after laparotomy with or without mechanical stimulation, whereas cisapride increased it after all three operations. Granisetron had no effect on the transit after the three operations when given alone. Prucalopride tended to increase the transit after laparotomy with or without mechanical stimulation when given alone. However, statistical significance was only reached when prucalopride was combined with granisetron. Erythromycin, a motilin receptor agonist, did not improve postoperative ileus in the rat.
CONCLUSIONS Cisapride, but not metoclopramide or erythromycin, is able to improve postoperative ileus in the rat. The results suggest that a combination of 5-HT3 receptor antagonist and 5-HT4 receptor agonist properties may be required to obtain a beneficial effect on surgery induced ileus in the rat. Furthermore, they indirectly indicate that stimulation of the excitatory mechanisms is not able to overcome the inhibitory influence of the neural reflex pathways activated during abdominal surgery.
- ileus
- motilin
- cisapride
- metoclopramide
- 5-HT3 receptor
- 5-HT4 receptor
Abbreviation used in this paper
- 5-HT
- 5-hydroxytryptamine
Statistics from Altmetric.com
Substituted benzamides, such as metoclopramide and cisapride, are prokinetics which are often used to treat upper abdominal symptoms related to delayed gastric emptying. These agents possess 5-hydroxytryptamine (5-HT3, serotonin) receptor antagonist and 5-HT4 receptor agonist properties.1 ,2Their antiemetic activity probably results from 5-HT3receptor antagonism.1-4 In addition, 5-HT3receptor antagonists are able to accelerate gastric emptying in some species such as the rat.5 ,6 Their prokinetic activity mainly results from 5-HT4 receptor agonism.1-4 The prokinetic benzamides probably enhance stomach motility in humans by enhancing cholinergic transmission possibly by stimulating neuronal 5-HT4 receptors. In the human colon, the benzamides cause relaxation of the circular colonic smooth muscles in vitro. Apparently in contrast, cisapride mildly stimulates lower gut motility and is moderately effective in the treatment of constipation. It is suggested that additional mechanisms may explain the effects of prokinetics on lower gut motility.2
5-HT4 receptor activation can cause relaxation or contraction depending on the region, cell type, and species under study. So far, our knowledge on the distribution and exact localisation of the 5-HT4 receptors in humans is limited. In human tissues, the effects of selective 5-HT4 receptor agonists suggest that these receptors are present on jejunal mucosa, ileal mucosa, gastric cholinergic neurones, and circular colonic muscles.1-3 In general, increased motor activity following 5-HT4 receptor activation results from increased release of acetylcholine from cholinergic neurones, and relaxation results from activation of 5-HT4 receptors on smooth muscle cells.7 In humans, mice, and dogs, selective 5-HT4 receptor agonists have been shown to accelerate colonic transit.4 ,8 ,9 They initiate a peristaltic reflex in humans and guinea pigs.7 ,10 In the rat gastrointestinal tract, 5-HT4 receptor agonists stimulate gastric emptying.2 ,3 ,11
Recently, a new 5-HT4 receptor agonist, prucalopride, was introduced.12 ,13 It is the first representative of the novel class of benzofurans, and is a highly specific and selective 5-HT4 receptor agonist. It has been shown to accelerate delayed gastric emptying and to induce giant migrating contractions in dogs.14 ,15 It has also been shown to shorten orocaecal and whole gut transit time in humans.16 These enterokinetic properties may be of great importance for the treatment of motor disorders characterised by decreased motility.
Postoperative ileus is a common complication after abdominal surgery and is defined as inhibition of the propulsive intestinal motility. It is generally accepted to result from activation of inhibitory neural reflex pathways involving inhibitory adrenergic neurones.17 We have previously shown the involvement of adrenergic and nitrergic neurones in the pathogenesis of postoperative ileus in the rat: a combination of the adrenergic neurone blocking drug reserpine and the nitric oxide synthase inhibitorl-nitroarginine was able to completely reverse the inhibition of the transit induced by a laparotomy plus mechanical stimulation of the gut.18 In this study, we investigated whether stimulation of excitatory pathways could overcome these inhibitory reflex pathways and eventually resolve postoperative ileus. Therefore we evaluated the effect of the enterokinetic prucalopride and compared its action with that of the clinically used prokinetics cisapride and metoclopramide. We also compared its effect with that of erythromycin, the model compound for a new class of prokinetics, the motilides, which are at present under development.1Cisapride is a more potent prokinetic agent than metoclopramide and is devoid of antidopaminergic activity. They both increase the release of acetylcholine from the postganglionic nerve endings in the myenteric plexus by activation of a neural 5-HT4receptor.1 ,19 ,20 Erythromycin, a macrolide antibiotic, has been shown to be a motilin receptor agonist.21 ,22Synthetic analogues of erythromycin, the motilides, are devoid of antibacterial properties and they represent a new class of prokinetic agents.1
Materials and methods
EXPERIMENTAL PROTOCOL
All procedures received approval from the commission for medical ethics at the University of Antwerp. Male Wistar rats (145–235 g) were fasted for 48 hours with free access to water. The operation protocol has previously been described in detail.18 Briefly, the rats were randomly divided into three groups and received an abdominal operation under ether anaesthesia. We have previously shown that ether anaesthesia has no effect on gastrointestinal transit in our rat model of ileus.18 In the first group, an abdominal skin incision was made after the abdomen had been shaved and disinfected. The second group had a laparotomy consisting of an incision through the abdominal skin, abdominal muscle layers, and peritoneum. The third group had a laparotomy followed by evisceration and mechanical stimulation of the small intestine and caecum. After the operations, the rats were allowed to recover for one hour. They then received an intragastric injection of 0.1 ml Evans blue (50 mg in 1 ml 0.9% NaCl)23 through a specially designed orogastric cannula introduced through the mouth. After 20 minutes, the rats were killed under ether anaesthesia and intestinal transit was measured as the migration of Evans blue from the pylorus to the most distal point of migration and expressed as distance (cm) migrated by the stain.
In a first series of experiments, the effect of two prokinetic agents, metoclopramide and cisapride, was tested on intestinal transit of Evans blue. The drugs were injected before the operation in an attempt to prevent development of postoperative ileus. The rats were randomly divided into three groups. The first group served as a control and received an intravenous injection of vehicle in a tail vein. They then underwent a skin incision, laparotomy, or laparotomy plus mechanical stimulation. The second group received an intravenous injection of metoclopramide 30 mg/kg one minute before the operation. The third group received an intravenous injection of cisapride 1 mg/kg one minute before the operation. The dose inducing 50% of the maximum effect (ED50) for stimulation of gastric emptying in the rat has previously been shown to be 1–1.5 mg/kg for cisapride and approximately eight times higher for metoclopramide.5 ,24However, in preliminary experiments, no prokinetic effect of metoclopramide 10 mg/kg could be demonstrated in control rats (data not shown), therefore we increased the dose to 30 mg/kg.
In a second series of experiments, we tested the effect of the 5-HT3 receptor antagonist granisetron. The rats were divided randomly into three groups. Rats in the first group served as a control and were injected with vehicle one minute before the operation. The second group was injected intravenously with granisetron 10 μg/kg and the third group with granisetron 50 μg/kg one minute before the operation. The ED50 value for stimulation of gastric emptying in rats for granisetron is 10 μg/kg.5
In a third series of experiments, we tested the effect of the selective 5-HT4 receptor agonist, prucalopride.12 ,13Prucalopride (R093877/R108512) is a newly synthesised enterokinetic agent and a benzofuran derivative with the chemical structure 4-amino-5-chloro-2,3-dihydro-N-[1(3-methoxypropyl)-4-piperidinyl]- 7-benzofurancarboxamide monochloride. The rats were divided randomly into three groups. The first group received an intravenous injection of vehicle and served as a control. The second group was injected intravenously with prucalopride 1 mg/kg and the third group with prucalopride 5 mg/kg one minute before the operation. The dose of prucalopride was based on gastric emptying studies using a non-caloric meal in rats (data on file at Janssen Research Foundation, Beerse, Belgium).
In a fourth series of experiments, we tested the effect of a combination of the 5-HT3 receptor antagonist and the 5-HT4 receptor agonist on intestinal transit in rats. The rats were divided randomly into two groups. Rats in the first group served as a control and were injected intravenously with vehicle. The second group received an intravenous injection of granisetron 50 μg/kg immediately followed by an intravenous injection of prucalopride 1 mg/kg one minute before the operation.
In a fifth series of experiments, the effect of erythromycin, a motilin receptor agonist,21 was tested on intestinal transit of Evans blue. The rats were randomly divided into two groups. Rats in the first group served as a control and received an intravenous injection of vehicle in a tail vein. They then had a skin incision, laparotomy, or laparotomy plus mechanical stimulation. The second group received an intravenous injection of erythromycin 1 mg/kg one minute before the operation. This dose has previously been shown to induce a prokinetic effect in dogs, rabbits, and humans.25-27
CHEMICALS USED
The following chemicals were used: diethyl ether,l-ascorbic acid (Merck, Darmstadt, Germany), erythromycin lactobionate (Erythrocine; S A Abbott, Saint-Remy, France), Evans blue (Sigma, St Louis, Missouri, USA), granisetron hydrochloride (Kytril; Smithkline Beecham Pharma, Genval, Belgium), metoclopramide hydrochloride (Alpha Pharma, Zwevegem, Belgium), NaCl 0.9% (Plurule) and sterile water (Baxter, Lessines, Belgium). Granisetron was kindly provided by Dr J Dierckens (Smithkline Beecham Pharma). Cisapride (R051619) and prucalopride (R093877/R108512) were kindly provided by J S (Janssen Research Foundation). Prucalopride was dissolved in sterile water, and cisapride was dissolved in 0.57 M ascorbic acid. All other drugs were dissolved in 0.9% NaCl.
PRESENTATION OF RESULTS AND STATISTICAL ANALYSIS
The total length of the small intestine was not statistically different between the groups (data not shown). Therefore results are expressed as distance (cm) migrated by Evans blue. The measurements were made from the pylorus to the most distal point of migration. Group differences were assessed by simple factorial analysis of variance followed by unpaired Student’s t test or by one way analysis of variance followed by the Bonferroni test for multiple comparisons. Values are shown as mean (SEM). p⩽0.05 was considered to be significant. All data were analysed with the SPSS for windows software (SPSS Inc, Chicago, Illinois, USA).
Results
EFFECT OF METOCLOPRAMIDE AND CISAPRIDE ON INTESTINAL TRANSIT
In control rats, transit after skin incision was 57.8 (2.1) cm (n = 10). It was significantly decreased by laparotomy to 34.6 (2.4) cm (n = 9). This inhibition of transit was even more pronounced after laparotomy plus mechanical stimulation (19.4 (2.4) cm, n = 9; fig 1).

Effect of skin incision (SI), laparotomy (LAP), or laparotomy plus mechanical stimulation of the small intestine and caecum (L+M) on intestinal transit in control rats (n = 9–10) and rats treated with metoclopramide (30 mg/kg; n = 9) or cisapride (1 mg/kg; n = 9–10). Results are expressed as cm migration of Evans blue and shown as mean (SEM). *Significantly different from the transit in control rats with the same operation (p⩽0.05); †significantly different from the transit in rats treated with metoclopramide with the same operation (p⩽0.05) (one way analysis of variance followed by the Bonferroni test).
Metoclopramide 30 mg/kg significantly increased transit after skin incision from 57.8 (2.1) cm (n = 10) in control rats to 71.3 (3.5) cm (n = 9) (fig 1). However, it further inhibited transit after laparotomy with or without mechanical stimulation: after laparotomy, transit was 20.8 (2.4) cm in rats treated with metoclopramide compared with 34.6 (2.4) cm in control rats, and after laparotomy plus mechanical stimulation, transit was 7.6 (1.6) cm in rats treated with metoclopramide compared with 19.4 (2.4) cm in control rats (n = 9, fig1).
Cisapride 1 mg/kg significantly increased transit after the three operations. It was 71.4 (2.6) cm (n = 9) after the skin incision, 51.6 (2.9) cm (n = 10) after laparotomy, and 28.9 (3.1) cm (n = 10) after laparotomy plus mechanical stimulation (fig 1).
The significant differences between the transit after skin incision and that after laparotomy with or without mechanical stimulation remained significant in the different treatment groups. Also the difference between transit after laparotomy and that after laparotomy plus mechanical stimulation remained significant in the three different groups.
EFFECT OF GRANISETRON ON INTESTINAL TRANSIT
Granisetron had no effect on transit after the skin incision, laparotomy, or laparotomy plus mechanical stimulation. Transit after skin incision tended to increase but statistical significance was not reached: transit was 61.4 (4.0) cm (n = 10) in control rats, 65.6 (4.3) cm (n = 9) in rats treated with granisetron 10 μg/kg, and 68.7 (4.0) cm (n = 10) in rats treated with granisetron 50 μg/kg (fig 2). Granisetron at a dose of either 10 or 50 μg/kg had no significant effect on transit after laparotomy or laparotomy plus mechanical stimulation (n = 9, fig 2).

Effect of skin incision (SI), laparotomy (LAP), or laparotomy plus mechanical stimulation of the small intestine and caecum (L+M) on intestinal transit in control rats (n = 9–10) and rats treated with granisetron 10 μg/kg (n = 9) or 50 μg/kg (n = 9–10). Results are expressed as cm migration of Evans blue and shown as mean (SEM). One way analysis of variance could not detect any significant differences between the treatment groups.
The differences between transit after the skin incision and that after laparotomy with or without mechanical stimulation, as well as the difference between transit after laparotomy alone and that after laparotomy plus mechanical stimulation remained significant in the different treatment groups.
EFFECT OF PRUCALOPRIDE ON INTESTINAL TRANSIT
Prucalopride had no effect on transit after the skin incision at either dose (1 and 5 mg/kg) used. Transit was comparable with that (63.6 (3.7) cm) in control rats after skin incision (n = 9, fig 3). Transit after laparotomy was significantly increased by prucalopride 1 mg/kg from 37.4 (3.1) cm in control rats to 49.9 (2.8) cm (n = 9, fig3). However, the increase produced by the 5 mg/kg dose was not significantly different: the transit was increased to 45.6 (3.4) cm (n = 9, fig 3). The transit after laparotomy plus mechanical stimulation tended to increase after treatment with prucalopride, but statistical significance was not reached. The transit was 17.9 (2.4) cm in control rats, 20.6 (1.7) cm after treatment with prucalopride 1 mg/kg, and 23.9 (2.5) cm after treatment with prucalopride 5 mg/kg (n = 9, fig3).
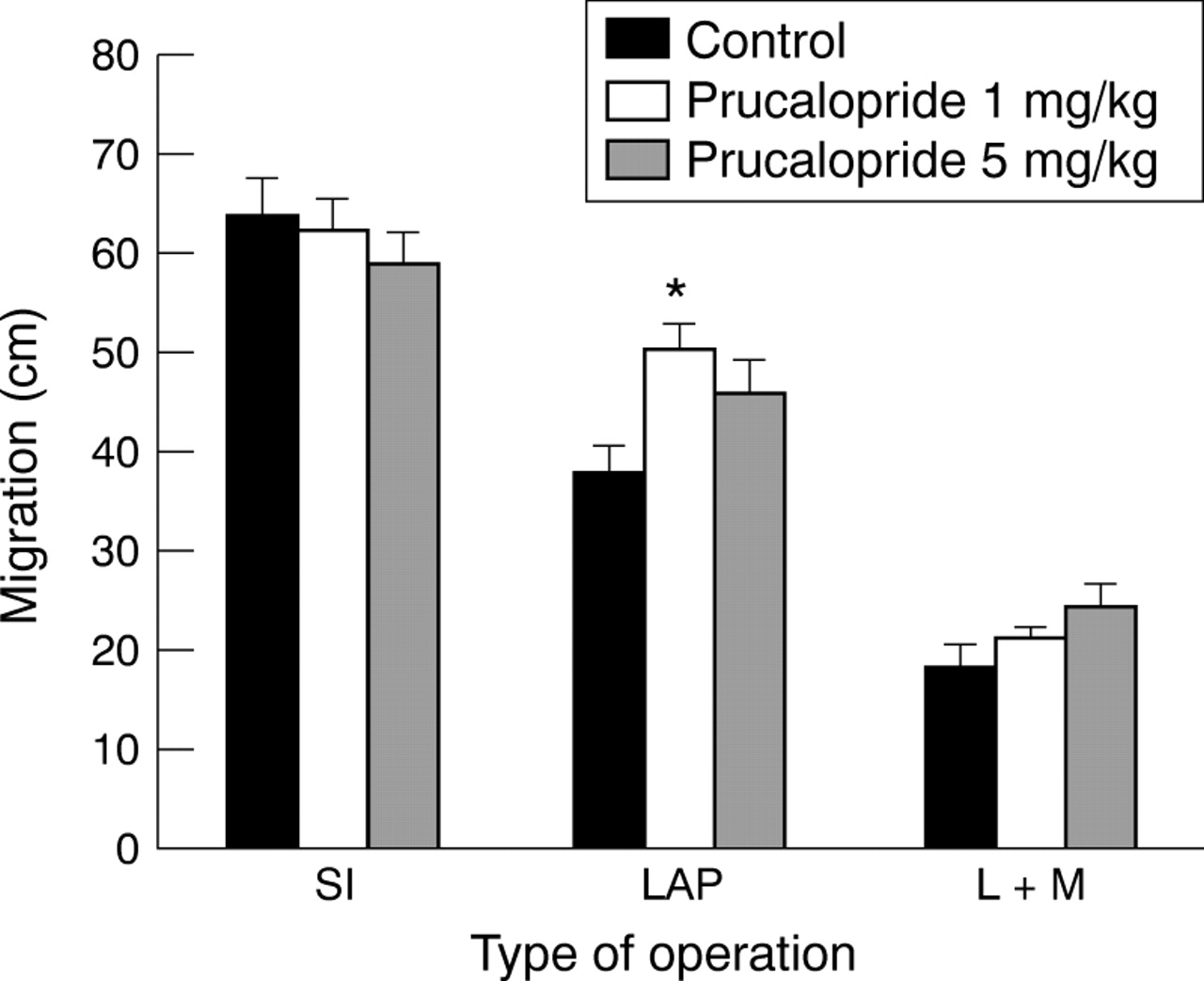
Effect of skin incision (SI), laparotomy (LAP), or laparotomy plus mechanical stimulation of the small intestine and caecum (L+M) on intestinal transit in control rats (n = 9) and in rats treated with prucalopride 1 mg/kg (n = 9) or 5 mg/kg (n = 9). Results are expressed as cm migration of Evans blue and shown as mean (SEM). *Significantly different from the transit in control rats after laparotomy (p⩽0.05) (one way analysis of variance followed by the Bonferroni test).
The differences between the transit after skin incision and that after laparotomy with or without mechanical stimulation, as well as the difference between the transit after laparotomy alone and that after laparotomy plus mechanical stimulation remained significant in the different treatment groups.
EFFECT OF A COMBINATION OF GRANISETRON AND PRUCALOPRIDE ON INTESTINAL TRANSIT
The combination of the 5-HT3 receptor antagonist granisetron (50 μg/kg) and the 5-HT4 receptor agonist prucalopride (1 mg/kg) had no effect on the transit after skin incision (n = 10, fig 4). However, the transit after laparotomy was significantly increased from 37.5 (2.8) cm in control rats to 45.5 (1.6) cm (n = 10, fig 4). Transit after laparotomy plus mechanical stimulation was also significantly increased by this treatment from 17.4 (2.2) cm (n = 10) in control rats to 24.6 (1.8) cm (n = 9) (fig4).

Effect of skin incision (SI), laparotomy (LAP), or laparotomy plus mechanical stimulation of the small intestine and caecum (L+M) on intestinal transit in control rats (n = 10) and rats treated with a combination of granisetron (50 μg/kg) and prucalopride (1 mg/kg) (n = 9–10). Results are expressed as cm migration of Evans blue and shown as mean (SEM). *Significantly different from the transit in control rats with the same operation (p⩽0.05) (unpaired Student’s t test).
In both groups, the differences between the transit after skin incision and that after laparotomy with or without mechanical stimulation and the difference between the transit after laparotomy alone and that after laparotomy plus mechanical stimulation remained significant, indicating that the combination treatment was not able completely to reverse the transit inhibition caused by the abdominal operations.
EFFECT OF ERYTHROMYCIN ON INTESTINAL TRANSIT
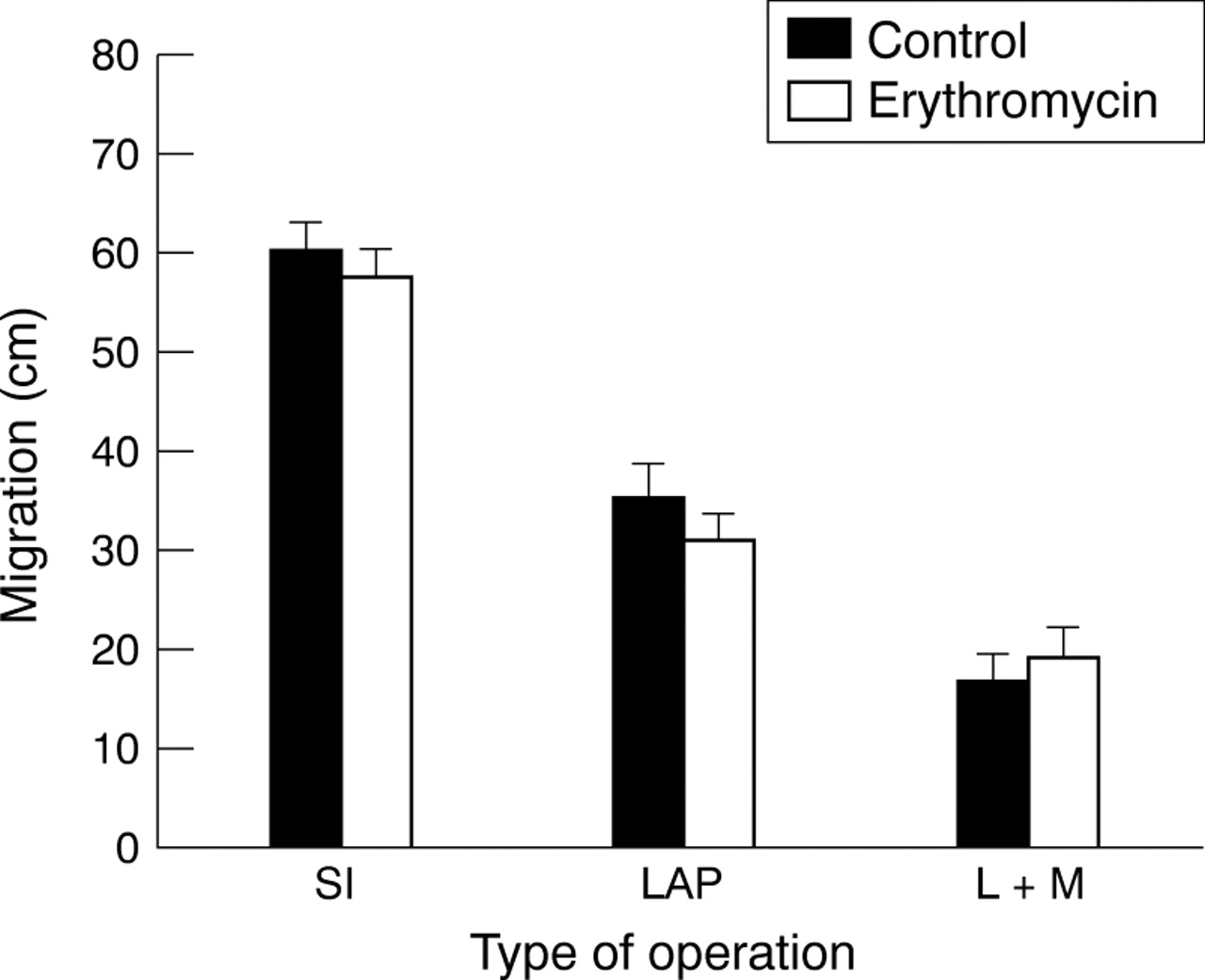
In control rats, transit after skin incision was 59.9 (3.0) cm. That after laparotomy was significantly decreased to 34.8 (3.9) cm. This transit inhibition was even more pronounced when the laparotomy was associated with mechanical stimulation of the intestine (16.2 (3.1) cm, n = 9; fig 5). Erythromycin 1 mg/kg had no effect on the transit after the three operations (n = 9, fig 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of skin incision (SI), laparotomy (LAP), or laparotomy plus mechanical stimulation of the small intestine and caecum (L+M) on intestinal transit in control rats (n = 9) and rats treated with erythromycin (1 mg/kg; n = 9). Results are expressed as cm migration of Evans blue and shown as mean (SEM). Unpaired Student’s t test could not detect any significant differences between the treatment groups.
The transit after the skin incision was significantly different from that after laparotomy with or without mechanical stimulation in both groups. Also the difference between the transit after laparotomy and that after laparotomy plus mechanical stimulation was significant in both groups.
Discussion
In our rat model of postoperative ileus, different degrees of inhibition of intestinal transit were achieved by different degrees of nociceptive stimulation. Skin incision had no effect on the transit, whereas it was significantly delayed by laparotomy. This inhibition was even more pronounced when the laparotomy was associated with mechanical stimulation of the gut, confirming earlier data obtained by Buenoet al.28 The role of inhibitory adrenergic neurones in the pathogenesis of postoperative ileus is generally accepted,17 but here we also show the involvement of inhibitory nitrergic neurones.18 In this study, we investigated the effect of prokinetic treatment on postoperative ileus in the rat. Although activation of 5-HT4 receptors is believed to be the mechanism of action of substituted benzamides,1 ,2 the newly synthesised 5-HT4 receptor agonist prucalopride did not improve recovery of postoperative ileus. Only combined 5-HT4receptor agonism and 5-HT3 receptor antagonism, provided by either cisapride or a combination of granisetron and prucalopride, increased transit significantly after laparotomy with or without mechanical stimulation.
The selective 5-HT4 receptor agonist, prucalopride,12 ,13 has been shown to induce giant migrating contractions and accelerate gastric emptying in dogs, and to stimulate gastrointestinal transit and bowel habits in healthy volunteers.14-16 However, in this study in the rat, prucalopride only tended to increase transit after laparotomy with or without mechanical stimulation, suggesting species differences. The effect of prucalopride is not clearly dose related, with only the lower dose significantly increasing transit after laparotomy. This lack of a dose related effect was also shown with other selective 5-HT4 receptor agonists in a model of gastric emptying in the rat and dog11 and in a model of canine colonic transit.4 Hypothetically, the fact that prucalopride is a partial agonist may explain the different effects of cisapride and prucalopride. However, the lack of a dose related effect of prucalopride does not support this hypothesis. Granisetron, a 5-HT3 receptor antagonist, was not able to increase intestinal transit after the three operations when given alone, although it was used at a concentration equal to the ED50value for gastric emptying in the rat.5 Whereas 5-HT3 receptor antagonists were previously shown to increase gastric emptying in rats,5 ,6 in our study granisetron only tended to increase transit after skin incision, but statistical significance was not reached. In contrast, the combination of granisetron and prucalopride significantly increased transit after laparotomy with or without mechanical stimulation. Therefore we hypothesise that both 5-HT3 receptor antagonism and 5-HT4 receptor agonism are required to reduce experimental ileus in the rat. The effect of cisapride resembles that of the granisetron and prucalopride combination on transit after laparotomy with or without mechanical stimulation. As cisapride is known to possess both 5-HT3 receptor antagonist and 5-HT4 receptor agonist properties, this finding may confirm our hypothesis. Several clinical studies have already shown a beneficial effect of repeated intravenous administration of cisapride on postoperative ileus,29-31 while other studies could not confirm this effect.32 ,33 Possibly, the effectiveness of cisapride in the resolution of postoperative ileus depends on the route of administration.34 A recent study in humans indicates that cisapride has prokinetic properties only when administered after the reappearance of the migrating motor complexes.35 In this study, cisapride was administered after the operation through a nasointestinal tube and it induced irregular spike bursts.
Interestingly, we found a differential effect of metoclopramide and cisapride on the abdominal surgery induced decrease in transit: metoclopramide further inhibited, whereas cisapride ameliorated the inhibition of, transit after laparotomy with or without mechanical stimulation. In a clinical randomised double blind study, Jepsenet al 36 also demonstrated this unexpected negative effect of metoclopramide on postoperative ileus; they proposed that it was due to the generation of uncoordinated non-propulsive peristalsis.36 The difference between metoclopramide and cisapride could be related to different affinities for the 5-HT3 receptor and the 5-HT4 receptor or to the central dopamine antagonistic activity of metoclopramide that is lacking for cisapride.19 ,20 On the other hand, recent reports suggest that cisapride enhanced gastroduodenal motility in the interdigestive state by increasing the plasma levels of motilin,37 suggesting that cisapride may enhance gastrointestinal motility by both serotonergic and non-serotonergic mechanisms. The latter may also explain the different effect of cisapride and the combination of prucalopride and granisetron on the transit after skin incision.
Erythromycin, a motilide, had no effect on transit in either normal conditions or after abdominal surgery. Similarly, Plourdeet al 38 could not show any improvement in gastric emptying in the rat after abdominal surgery even if the rats were treated with a higher concentration (40 mg/kg) of erythromycin. Although erythromycin induced an increase in the motility index of the small intestine in the rat in one study,39several other studies failed to show a prokinetic action of erythromycin in the rat.21 ,22 These results may suggest that the rat is not an ideal species in which to study the effects of motilides, although motilin immunoreactivity has been shown in the rat small intestine.22 In humans also, treatment with erythromycin did not alter the clinical variables of gastrointestinal motility after abdominal surgery,40 despite the acceleration of gastric emptying in healthy subjects41 and in patients with diabetic gastroparesis.42 ,43 Therefore the efficacy of erythromycin or other motilides in the treatment of postoperative ileus remains to be proved.
In conclusion, of the prokinetics studied, only cisapride is of use in the treatment of postoperative ileus. Our study suggests that a combination of 5-HT3 receptor antagonist and 5-HT4 receptor agonist properties may be required to obtain a beneficial effect on surgery induced ileus in the rat. Although prokinetics have a beneficial effect in the treatment of gastric emptying disorders, they may be of limited use in the treatment of postoperative ileus. Their clinical relevance remains to be proved. Our results indirectly indicate that stimulation of excitatory neurones is not able to overcome completely the inhibitory influence of the neural reflex pathways activated by abdominal surgery. However, it is worth investigating further the effects of novel enterokinetics that have profound effects on colonic motility in humans.
Acknowledgments
B De W is a research assistant of the Fund for Scientific Research—Flanders (FWO), Belgium. This work was supported by the FWO—Flanders, Belgium (grant no G.0220.96) and by the Interuniversity Pole of Attraction Programme (grant no P4/16, Services of the Prime Minister—Federal Services for Scientific Technical and Cultural Affairs). The authors wish to thank Mrs L Van de Noort for typing the manuscript.
Abbreviation used in this paper
- 5-HT
- 5-hydroxytryptamine