Article Text

Abstract
Background: Glucagon-like peptide-1(7–36)amide (GLP-1) retards gastric emptying, reduces food intake, and inhibits antroduodenal and stimulates pyloric motility.
Aims: To assess the effects of synthetic GLP-1 on fundus tone and volume waves, gastric compliance, and perception of gastric distension.
Subjects: Eleven healthy male volunteers.
Methods: Background infusions were saline, or GLP-1 at 0.3 or 0.9 pmol/ kg/min on separate days in random order. Interdigestive fundus motility was recorded by barostat (maximum capacity of intragastric bag 1200 ml) during basal and peptide periods of 60 minutes each. Thereafter stepwise isobaric distensions were performed with ongoing peptide infusion, and gastric sensation was scored.
Results: Low and high loads of GLP-1 induced physiological and supraphysiological plasma immunoreactivities, respectively. GLP-1 dose dependently diminished fundus tone (162.9 (15.0) and 259.5 (17.2) v 121.1 (6.0) ml with saline; p<0.0001). It greatly reduced volume waves and total volume displaced by these events (p<0.0001). Gastric compliance derived from isobaric distension rose in a dose related manner (42.6 (5.5) and 63.6 (7.7) v 27.0 (3.5) ml/mm Hg; p=0.0004) with a concomitant reduction of the pressure at half maximum bag volume (6.4 (0.4) and 5.5 (0.4) v 7.2 (0.1) mm Hg; p<0.0001). GLP-1 did not change perception of isobaric distension but reduced the perception score related to corresponding bag volume (p<0.0001).
Conclusions: GLP-1 is a candidate physiological inhibitory regulator of fundus motility. It allows the stomach to afford a larger volume without increase in sensation.
- barostat
- gastric compliance
- gastric tone
- isobaric distension
- volume waves
- CCK, cholecystokinin
- GLP-1, glucagon-like peptide-1(7-36)amide
- IR, immunoreactive
- MDP, minimal distending pressure
- PP, pancreatic polypeptide
Statistics from Altmetric.com
- CCK, cholecystokinin
- GLP-1, glucagon-like peptide-1(7-36)amide
- IR, immunoreactive
- MDP, minimal distending pressure
- PP, pancreatic polypeptide
Derived from proglucagon, glucagon-like peptide-1(7–36)amide (GLP-1) is an intestinal hormone released from L cells in response to lipid and, especially, carbohydrate stimulation. A threshold duodenal delivery of glucose exceeding approximately 1.4 kcal/min is required to elicit GLP-1 release.1 The predominant localisation of the L cells in the distal small bowel appears to contrast with the rapid postprandial release of the peptide.2 However, rat and human experiments perfusing lipid into the jejunum argue in favour of intraluminal nutrient exposure of jejunal L cells as the major mechanism of GLP-1 release.3, 4 One target of this peptide is the endocrine pancreas where it exerts a glucose dependent insulinotropic effect and lowers glucagon release.5 In humans, even in the fasting state, the pancreatic A cell is under a tonic inhibitory control by GLP-1. With physiological hyperglycaemia even basal circulating concentrations of this peptide stimulate insulin release.6 Both in healthy subjects and in patients with type 2 diabetes mellitus, GLP-1 lowers postprandial glycaemic excursion by the interplay of retarded gastric emptying, stimulated insulin, and inhibited glucagon release.7, 8 Moreover, GLP-1 in patients with impaired glucose tolerance restores the ability of the pancreatic B cell to sense and respond to subtle changes in blood glucose.9 Furthermore, GLP-1 reduces food intake both in healthy subjects and in obese patients with type 2 diabetes.10, 11 These combined effects improve glucose tolerance and indicate its therapeutic potential in the treatment of diabetes mellitus and prediabetic conditions.8, 12
Apart from its effects on glucose homoeostasis and food intake, GLP-1 profoundly affects motor and secretory functions of the proximal gastrointestinal tract. Postprandial GLP-1 plasma levels almost abolish antral and duodenal contractile activity whereas pyloric tone and the frequency of isolated pyloric pressure waves increase.13 GLP-1 is a candidate physiological inhibitory modulator of antral and duodenal motility and a candidate stimulatory regulator of the pylorus. Moreover, this peptide inhibits gastric acid and pancreatic enzyme secretion.7, 14
The tone of the proximal stomach is involved in gastric emptying of liquids and especially in the generation of dyspeptic symptoms.15 Disturbed gastric accommodation to a meal has been implicated in the generation of symptoms both in functional and diabetic dyspepsia.16, 17 The effect of GLP-1 on motor and sensory function of the fundus is unknown. Thus this study was designed to assess tonic and phasic motor responses of the fundus to GLP-1 and to elucidate perception of isobaric distensions with and without the peptide. The conceptual background of these experiments was to look for fundus motor correlates of retarded gastric emptying with GLP-1 and to assess the interplay of gastric relaxation and induction of dyspeptic symptoms under gastric distension.
MATERIAL AND METHODS
Subjects
Eleven healthy male volunteers, aged 22–28 years and within 10% of ideal body weight, participated in the studies. None was taking medication, and none suffered from gastrointestinal symptoms or any systemic disease. The studies were approved by the ethics committee of the Medical Faculty of the Philipps University of Marburg, and all participants provided written informed consent.
Gastric barostat
An electronic barostat (Distender Series II; G&J Electronics, Toronto, Canada) was used to assess the volume of the proximal stomach under a constant pressure clamp and to perform isobaric distensions. A polyethylene bag (1200 ml maximum capacity) was tied to the end of a double lumen polyvinyl tube (ID 4 mm, OD 5 mm). The polyethylene bag was infinitely compliant at the inflation volumes observed in this study. The barostat was set to maintain a fixed pressure level in the intragastric bag by electronic feedback regulation of air volume in the bag. Pressure and volume levels were controlled and recorded by a computer program (Protocol Plus; G&J Electronics, Toronto, Canada) running on a standard IBM compatible PC connected to the barostat.
Experimental protocol
All studies were performed after an overnight fast. Three experiments separated by at least one week were performed in each subject in random order with subjects blinded for the load of peptide or saline being infused.
Placement of intragastric bag
The intragastric bag was finely folded and introduced through the mouth into the stomach. To unfold the bag, it was manually filled with 300 ml of air. The catheter was pulled back carefully until its passage was restricted by the lower oesophageal sphincter. The tube was then introduced a further 2 cm. Correct position was checked fluoroscopically. Thereafter the bag was deflated and connected to the barostat. Subjects were resting comfortably in an approximately 70° erect position. Indwelling catheters were inserted into antecubital veins of opposite arms for intravenous infusions and blood sampling, respectively.
Minimal distending pressure
The minimal distending pressure (MDP) is the pressure needed to overcome the intra-abdominal pressure. This is defined as the first pressure level that provides an intragastric bag volume of more than 30 ml.15 It was determined by increasing intrabag pressure in steps of 1 mm Hg every minute. Thereafter, intrabag pressure was set at MDP+1 mm Hg during a 15 minute equilibration period before recording of gastric tone was started.
Infusion periods
On each study day a basal period of 60 minutes was followed by a 95 minute infusion period with intravenous saline or GLP-1 at 0.3 or 0.9 pmol/kg/min. These peptide loads were chosen to obtain physiological postprandial and supraphysiological plasma levels, respectively.13 During the initial 10 minutes of each infusion period, GLP-1 was infused at double doses (0.6 and 1.8 pmol/kg/min, respectively) to quickly establish steady state plasma levels.13 Thus the infusion period was divided into an initial 20 minutes of loading and a subsequent 75 minute steady state period. The first 60 minutes of the latter period were devoted to recording of gastric tone and the last 15 minutes to isobaric distensions.
Measurement of gastric tone
The barostat was set to maintain a pressure of MDP+1 mm Hg. Gastric tone was continuously recorded during basal, loading, and steady state periods.
Isobaric distension
After having recorded gastric tone, stepwise isobaric distensions were performed at 1, 2, 4, 6, and 8 mm Hg above MDP with each distension lasting for two minutes. Distension was stopped immediately if a volume of 800 ml was exceeded or if the participant could not tolerate further distension. MDP+8 mm Hg was the maximum intrabag pressure tolerated by all volunteers in experiments with GLP-1.
Gastric sensation
During isobaric distensions participants were advised to report their perception of upper abdominal sensations induced by each distending step on a scale graded from 1 to 6. The scale referred to verbal descriptors defining scores as follows: 1, no perception; 2–4, mild, definite, and strong perception, respectively; 5, discomfort; and 6, painful sensation. A score of 6 resulted in immediate termination of the distension. Subjects were advised to consider intervals between different scores as equal. Perception was rated 90 seconds after initiation of each distension step.
Blood sampling
Blood samples were obtained throughout the experiment at 0, 15, 30, 45, 60, 80, 95, 110, 125, and 140 minutes after the start of the basal period, with 80 minutes representing the start of the steady state period. Small aliquots were immediately used to measure blood glucose whereas blood samples for later determination of immunoreactivities of gastrointestinal peptides were collected in ice chilled EDTA tubes containing 1000 kallikrein inhibiting units of aprotinin per ml of blood and were immediately centrifuged. Plasma was stored at −20°C until assayed.
Analysis of gastric motility and sensation
Gastric tone and volume waves
Pressure and volume of the barostat bag were sampled as digital signals at a frequency of 1 Hz. Volume data were automatically corrected for air compressibility by the operating software of the barostat. A computer algorithm eliminated motion and respiratory artefacts and detected volume waves representing phasic volume variations. Volume waves were defined as changes in volume >30 ml that reverted in less than two minutes to a volume within 50% of the previous level.18 Volume waves were defined as start and end if their slope exceeded and fell below 1.9 ml/s, respectively. Their amplitude was measured from baseline to peak. Gastric tone was represented by baseline bag volume—that is, mean bag volume excluding volume waves—and expressed as mean value per 15 minutes. Correspondingly, the number of volume waves and volume wave index were given for subsequent 15 minute intervals. The volume wave index was defined as the area under volume waves over baseline, the latter representing gastric tone.
Gastric compliance
For each distension step all volume data of the respective two minute recording period were averaged to determine volume accommodation. The pressure-volume relationship during isobaric distension is often non-linear. It is characterised by an initial flat portion, a transition to a steeper segment at an inflection point, and a flatter segment at high pressures.19 Two models were used to calculate gastric compliance (ΔV/ΔP). Firstly, absolute ΔV values were plotted against ΔP. Here, compliance was defined as VMDP+8 mm Hg−Vinflection point/ΔP with the inflection point being derived visually. This model defines compliance as the linear slope of the curve after the inflection point referring to the viscoelastic properties of the gastric wall. Secondly, the compliance curves for each experiment and each subject were fitted to a power exponential model20 using non-linear least squares regression:  . rP is the reciprocal pressure (1/pressure), R is the ratio of initial volume at starting pressure, Vmax is the maximum volume at maximum pressure, and pV is the proportionate volume (V/Vmax). pV−R refers to the proportionate increase in bag volume compared with the volume at the starting pressure of MDP+1 mm Hg. γ is an estimate of the overall shape of the curve, and σ is the instantaneous slope of the change in volume as a function of 1/pressure. The estimated γ and σ values were used to calculate the pressure above MDP corresponding to half maximum volume with
. rP is the reciprocal pressure (1/pressure), R is the ratio of initial volume at starting pressure, Vmax is the maximum volume at maximum pressure, and pV is the proportionate volume (V/Vmax). pV−R refers to the proportionate increase in bag volume compared with the volume at the starting pressure of MDP+1 mm Hg. γ is an estimate of the overall shape of the curve, and σ is the instantaneous slope of the change in volume as a function of 1/pressure. The estimated γ and σ values were used to calculate the pressure above MDP corresponding to half maximum volume with  . In this model, reduction of P½ and σ reflect an increase in compliance. To assess the goodness of fit to the non-linear curves, the fraction of variance in the data which can be accounted for by the fitted curve was computed for each individual curve according to R2=1−(residual sum of squares/total sum of squares), where the total sum of squares is n−1 times the square of the standard deviation of the observed fractions.1
. In this model, reduction of P½ and σ reflect an increase in compliance. To assess the goodness of fit to the non-linear curves, the fraction of variance in the data which can be accounted for by the fitted curve was computed for each individual curve according to R2=1−(residual sum of squares/total sum of squares), where the total sum of squares is n−1 times the square of the standard deviation of the observed fractions.1
Gastric sensation
Perception scores at each distension step were documented. Moreover, we calculated cumulative scores as the sum of perception scores at all distensions steps.
GLP-1(7–36)amide
Synthetic GLP-1(7–36)amide was purchased from Polypeptide Laboratories (Wolfenbüttel, Germany). The preparation was delivered with a peptide content of 87.1% and a peptide purity >99%. It was dissolved in 1% human serum albumin, filtered through 0.2 μm nitrocellulose filters, and thereafter stored at −70°C.13 Samples were tested for pyrogens and bacterial growth, and no contamination with bacterials or endotoxins was detected. Dose calculations were based on peptide content rather than weight of preparations.
Determinations and assays
Blood glucose concentrations were measured using a glucose analyser employing the glucose oxidase method (YSI 1500 G; Schlag, Bergisch-Gladbach, Germany) with a coefficient of variation of <2%. Plasma insulin was measured by the Abbott Imx Microparticle Enzyme Immunoassay, with an average intra-assay coefficient of variation of 5%. Plasma immunoreactivities of C peptide, glucagon, and pancreatic polypeptide (PP) were analysed by commercially available radioimmunoassay kits (Biermann, Bad Nauheim, Germany and Euradiagnostica, the Netherlands). Immunoreactive (IR) GLP-1 was measured using the specific polyclonal antibody GA 1178 (Affinity Research, Nottingham, UK) as previously described.1, 13 The detection limit of the assay was 0.25 pmol/l. The antiserum did not cross react with glucose dependent insulinotropic peptide, pancreatic glucagon, glicentin, oxyntomodulin, or GLP-2. Intra- and inter-assay coefficients of variation were 3.4% and 10.4%, respectively.
Statistical analysis
All group data are expressed as mean (SEM) unless normal distribution of data was rejected by the Komolgorov-Smirnov test. Time courses of gastric tone and phasic volume events as well as blood glucose and immunoreactivities of gastrointestinal peptides after saline and both loads of GLP-1 were compared by two way repeated measures analysis of variance. These analyses accounted for potential differences in baseline values on different days by employing incremental values over basal at each time point during the steady state period. Basal values were defined as the mean of all four 15 minute intervals in the basal period. In addition, for each of these parameters mean incremental or decremental values over basal during the steady state period were compared by one way repeated measures analysis of variance (see tables). Differences in perception scores and intrabag volumes during isobaric distension were analysed by two way repeated measures analysis of variance employing distension level and background infusion as factors. Cumulative perception scores and the parameters of compliance were compared by one way repeated measures analysis of variance. Each ANOVA was followed by a Student-Newman-Keuls multicomparison test if appropriate. Differences were considered significant at p<0.05.
RESULTS
Plasma immunoreactivities of gastrointestinal peptides and blood glucose
In the basal state, plasma IR-GLP-1 was almost identical on the three study days, approximating 2.5 pmol/l (fig 1A⇓, table 1⇓). After the loading period, both dosages of GLP-1 resulted in steady state plasma levels resembling physiological postprandial (low dose) and supraphysiological (high dose) levels, respectively. GLP-1 reduced fasting glycaemia to mean levels of 74.9 (2.0) and 67.4 (1.2) mg/dl (p<0.0001, two way repeated measures ANOVA) (fig 1C⇓) with the high load being more potent (table 1⇓). However, even the high load did not induce hypoglycaemia: the lowest single individual value was 48 mg/dl, the lowest mean individual value was 59.3 mg/dl, and no subject reported hypoglycaemic symptoms. GLP-1 only transiently stimulated insulin release during the loading period. This effect did not persist under steady state plasma levels of GLP-1 (p=0.235) (fig 1B⇓, table 1⇓). The same was true for C peptide which was only transiently increased by GLP-1 in the loading period (table 1⇓). The high dose of GLP-1 reduced PP release with mean IR-PP of 91.3 (15.7) compared with 112.8 (14.3) pg/ml under saline (p<0.05) (fig 1D⇓, table 1⇓).
Effect of glucagon-like peptide-1(7–36)amide (GLP-1) on blood glucose and plasma immunoreactivities of gastrointestinal peptides
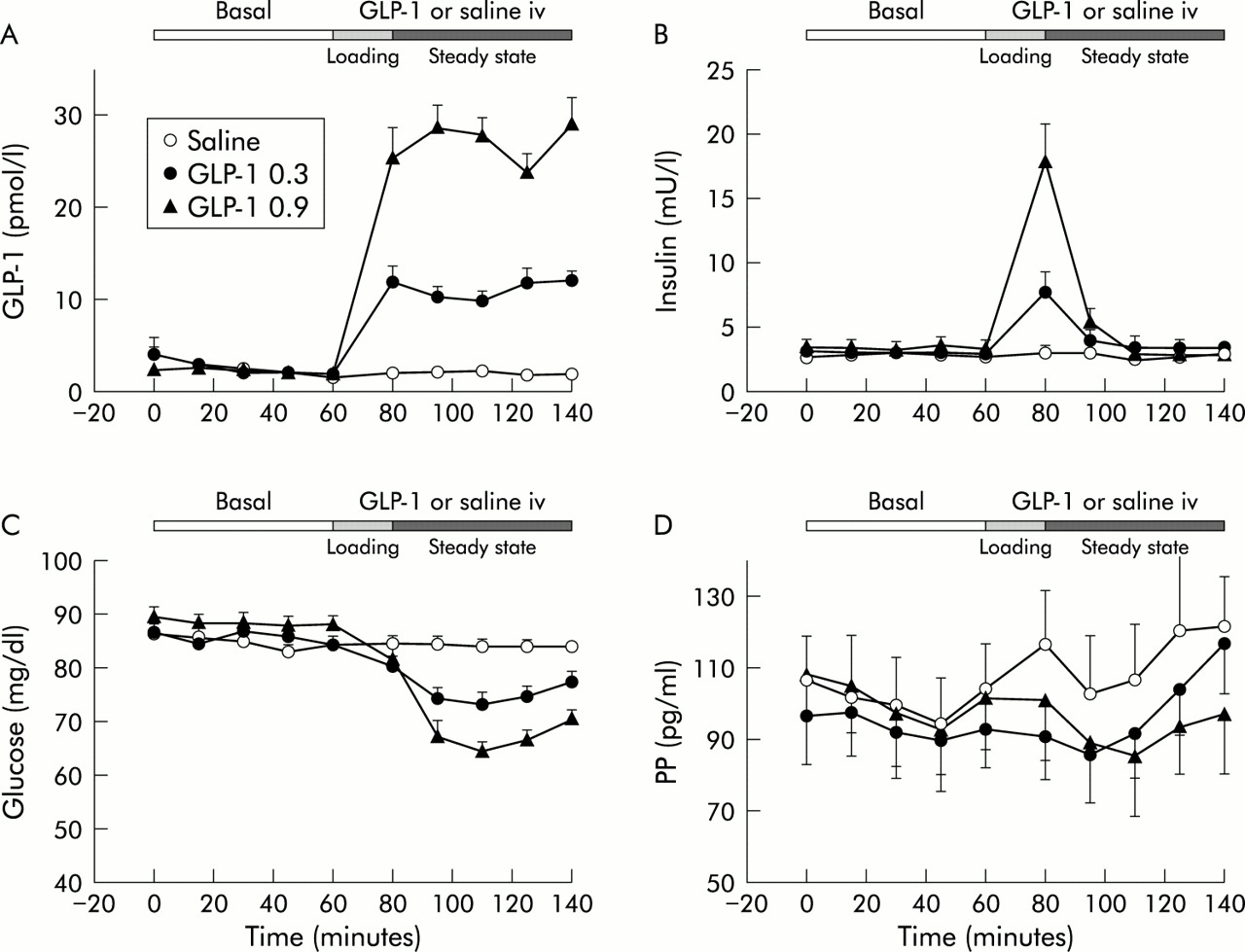
Effect of physiological (0.3 pmol/kg/min (0.3)) and supraphysiological (0.9 pmol/kg/min (0.9)) intravenous (iv) loads of glucagon-like peptide-1(7–36)amide (GLP-1) on blood glucose and plasma immunoreactivities of gastrointestinal hormones in 11 healthy volunteers. GLP-1 dose dependently reduced blood glucose (C) and increased immunoreactive (IR)-GLP-1 (A) (p<0.0001; two way repeated measures ANOVA). IR-insulin was unaltered during steady state infusion. Only the high GLP-1 load reduced IR-pancreatic polypeptide (PP) (p<0.05).
Gastric tone
In the fasting state, basal gastric tone was almost identical on the three study days, approximating 100 ml before starting the infusions of saline, or low or high loads of GLP-1 (figs 2, 3A⇓⇓, table 2⇓). GLP-1 distinctly increased intragastric bag volume reflecting relaxation of the gastric fundus (p<0.0001, two way repeated measures ANOVA). Increasing the peptide load markedly enhanced the effect. Relaxatant effects of GLP-1 compared with basal volume averaged 61.3% for the low and 160.4% for the high load (fig 3A⇓).
Effect of glucagon-like peptide-1(7–36)amide (GLP-1) on fundus motility and perception of isobaric distension

Original recording of intragastric bag volume in a sample subject. The baseline volume tracings denote fundus tone; phasic downward deflections exceeding 30 ml refer to volume waves. Glucagon-like peptide-1(7–36)amide (GLP-1) 0.3 pmol/kg/min (0.3) and 0.9 pmol/kg/min (0.9) dose dependently raised the baseline, representing a reduction in tone, and suppressed volume waves.

Effect of physiological (0.3 pmol/kg/min (0.3)) and supraphysiological (0.9 pmol/kg/min (0.9)) intravenous (iv) loads of glucagon-like peptide-1(7–36)amide (GLP-1) on fundus tone represented by bag volume (A), frequency of volume waves (B), and total volume displaced by these phasic events (volume wave index (C)) in 11 healthy volunteers. GLP-1 dose dependently relaxed the fundus and reduced both parameters characterising volume waves (p<0.0001; two way repeated measures ANOVA).
Volume waves
In the basal interdigestive state, volume waves occurred at a frequency of approximately one per minute (figs 2, 3B⇑⇑, table 2⇑). GLP-1 clearly reduced the occurrence of these phasic volume events (p<0.0001, two way repeated measures ANOVA) with the high load still exceeding the effect of the low. Decremental effects of GLP-1 averaged 33.6% and 65.5% for the low and high load, respectively. The volume wave index expressed as the area under the volume waves over baseline represented totally displaced volume by these phasic events. In line with the effects on frequency, GLP-1 clearly reduced the volume wave index (p<0.0001). This effect was dose dependent (fig 3C⇑, table 2⇑). Per cent reduction averaged 36.6% for the low and 71.6% for the high dose. The amplitude of the volume waves was significantly reduced by GLP-1 (p=0.0016) without any differences between loads (table 2⇑). Duration of volume waves remained unchanged.
Gastric distensions
Isobaric distension caused a non-linear increase in bag volume. The visually derived inflection point of the curves was 2 mm Hg above MDP in 30 experiments, and 4 mm Hg in three experiments (fig 4A⇓). The measured volume data during isobaric distension fitted well to the power exponential model with a median R2 of 0.983 and 25th and 75th percentiles of 0.956 and 0.991, respectively, estimating goodness of fit for the non-linear compliance curves. GLP-1 distinctly increased gastric compliance derived from isobaric distension (fig 4A⇓, table 2⇑). This effect was dose dependent. It was true for both modes calculating compliance—that is, the linear slope of the volume-pressure curve after the inflection point (p=0.0004, two way repeated measures ANOVA) and the instantaneous slope (σ) of the volume-pressure curve derived from the power exponential model (p<0.0001). Correspondingly, the pressure at which half the maximum volume was achieved decreased with GLP-1 (p<0.0001, one-way repeated measures ANOVA). However, the initial flat portion of the compliance curve before the inflection point remained unchanged.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of physiological (0.3 pmol/kg/min (0.3)) and supraphysiological (0.9 pmol/kg/min (0.9)) intravenous (iv) loads of glucagon-like peptide-1(7–36)amide (GLP-1) on compliance of the proximal stomach (A) and perception (B) of isobaric distensions in 11 healthy volunteers. GLP-1 dose dependently increased linear compliance defined as the linear slope after the inflection point of the curve (p=0.0004; (A) upper panel), and non-linear compliance derived from the power exponential model by increasing the slope of the curve (decreasing σ), and therefore reducing the pressure at half the maximum bag volume (P½) (p<0.0001; (A) lower panel). GLP-1 enhanced volume accommodation (p=0.0008) but did not influence perception (p=0.513; (B) upper panel). Therefore, the perception/volume relationship was dose dependently reduced with GLP-1 (p<0.0001; (B) lower panel). GLP-1 allowed the stomach to afford a greater volume without increase in perception. MDP, minimal distending pressure. *p<0.05 versus saline, †p<0.05 versus GLP-1 0.3 pmol/kg/min. Differences in compliance (A) were compared using one way repeated measures ANOVA and differences in perception (B) using two way repeated measures ANOVA.
GLP-1 did not affect the threshold of first perception which occurred at 4.5 (0.7), 3.6 (0.8), and 3.9 (0.6) mm Hg above MDP in experiments with saline, and low and high loads of GLP-1. Across all distension steps, GLP-1 dose dependently enhanced volume accommodation indicating gastric relaxation (p=0.0008, two way repeated measures ANOVA) (fig 4B⇑). However, GLP-1 did not significantly influence perception of isobaric distension (p=0.513 across all steps). The trend towards enhanced perception occurring at 6 and 8 mm Hg above MDP was not significant.
Stepwise increase in intragastric pressure raised both perception scores and bag volumes (fig 4B⇑, upper panel). However, GLP-1 dose dependently elicited a rightward shift of the volume/perception curve—that is, it enhanced relaxation but not perception. The relationship of perception to the corresponding volume remained fairly constant at the different distension levels with and without GLP-1. However, due to enhanced gastric volume accommodation without change in perception, the volume related perception was dose dependently lowered with GLP-1. This effect was maintained over all distension levels (p<0.0001, two way repeated measures ANOVA) (fig 4B⇑, lower panel).
Association of reduction in glycaemia and motor effects with GLP-1
Linear regression analysis was used to assess the putative contribution of lowered blood glucose to motor effects. The following relationships between reduction in glycaemia and motor phenomena were identified: gastric tone: R2=0.193, p=0.015; frequency of volume waves: R2=0.348, p<0.001; σ as non-linear measure of compliance: R2=0.179, p=0.039.
DISCUSSION
This is the first study which has assessed the effects of GLP-1 on the gastric fundus. The salient findings were as follows: (i) GLP-1 dose dependently relaxed the fundus; (ii) it greatly reduced phasic volume events; (iii) it increased gastric compliance; and (iv) across all isobaric distension steps it allowed the stomach to afford larger volumes without an increase in sensation.
The low load of GLP-1 infused in this study emulated approximately incremental IR-GLP-1 observed after an oral glucose load of 100 g.1 Thus this intravenous load reproduced postprandial plasma levels and may be considered physiological. As the low load of GLP-1 markedly relaxed the fundus and suppressed phasic volume events, this peptide is a candidate physiological inhibitory modulator of fundus motor activity. Experiments blocking the effects of endogenous GLP-1 both in the interdigestive state and postprandially utilising the specific GLP-1 receptor antagonist exendin(9–39)amide6 will further elucidate this issue. In humans, physiological plasma levels of both gastrin and cholecystokinin (CCK) have been shown to relax the fundus.21, 22 Here, the effect of gastrin was mediated by stimulation of gastric acid secretion.21 In terms of CCK, experiments with the CCK-A receptor antagonist loxiglumide revealed endogenous CCK to be a physiological inhibitory regulator of fundus tone.23 Our data support the notion that, apart from CCK, GLP-1 is another enterogastrone regulating the gastric fundus.
To understand the mechanism whereby GLP-1 affects gastric motility and sensation, endocrine and metabolic effects of this peptide have to be considered. Both hyperglycaemia and hyperinsulinaemia have been shown to induce motor patterns in the gastrointestinal tract associated with slow transit.4, 24–,26 Moreover, bolus injection of insulin results in gastric relaxation.27 However, with steady state GLP-1 infusion in the present study, hyperinsulinaemia was no longer present. Thus in our experiments GLP-1 mediated hyperinsulinaemia did not appear to be a relevant mechanism of gastric relaxation. Hyperglycaemia relaxes the fundus and enhances perception of gastric distension compared with euglycaemia both in interdigestive and postprandial states.25, 26 Overt hypoglycaemia also relaxes the fundus.27 However, in the present study, GLP-1 lowered fasting glycaemia without inducing overt hypoglycaemia. The level of glycaemia with the low load of GLP-1 in particular was outside the hypoglycaemic range, despite marked gastric motor effects. It has recently been established that changes in blood glucose concentration within the physiological postprandial range also affect gastrointestinal motor and sensory function.28 However, physiological changes in blood glucose have been shown not to affect gastric compliance and perception in normal subjects.29 In the present study, there were significant but only weak to moderate associations between blood glucose and all three motility parameters tested—that is, fundus tone, volume waves, and compliance σ—during the steady state period. The reduction of glycaemia accounted for less than 20% of the variance in fundus tone and compliance, and for 35% of the variance in volume wave frequency. Thus limited reduction of glycaemia with GLP-1 may contribute to motor effects but is not a predominant mechanism. Another endocrine mediator reducing fundus tone is pancreatic glucagon.30 However, since GLP-1 inhibits and does not stimulate glucagon release, this peptide does not mediate relaxatory effects of GLP-1 on the fundus.6–,8
GLP-1 neither changed basal muscle tone in smooth muscle strips from the gastric fundus and corpus in rats nor did it affect the length of smooth muscle cells isolated from rabbit antrum.31, 32 Thus a direct effect on gastric smooth muscle mediated via GLP-1 receptors located on these effector cells is highly unlikely. On the other hand, multiple findings support the notion that GLP-1 inhibits motor and secretory functions of the upper gastrointestinal tract by interfering with vagal neural input: GLP-1 almost abolished sham feeding induced gastric acid secretion, and its inhibitory effect on pentagastrin induced secretion depended on the integrity of the vagus nerve.14, 33 In a pig model, vagally stimulated gastropancreatic secretion and antral motility were strongly inhibited by GLP-1.34 The precise site of the inhibitory action of GLP-1 on vagal input to the gastrointestinal tract remains to be defined. However, it has been shown in rats that GLP-1 induced inhibition of gastric emptying involves a capsaicin sensitive pathway, indicating interaction with vagal afferent nerves.35 In addition, specific GLP-1 binding sites in various regions around the third ventricle in rats, in particular the subfornical organ and the area postrema, have been demonstrated which are accessible to GLP-1 from the systemic circulation.36, 37 Thus apart from interacting with vagal afferents, circulating GLP-1 may affect vagal pathways in the brainstem by acting as a humoral afferent. In the present study, inhibition of PP release with GLP-1 argues in favour of suppression of vagal cholinergic input as a mechanism of gastric relaxation because this hormone of the endocrine pancreas is under strong vagal cholinergic control. A direct action of GLP-1 on pancreatic PP cells or a paracrine effect via somatostatin seems unlikely as GLP-1 induces stimulation rather than inhibition of PP release from isolated human pancreatic islets.38 Preliminary data using the specific GLP-1 antagonist exendin(9–39)amide indicated that endogenously released GLP-1 increased postprandial fundus volume.39 Fundus contraction with the antagonist was fully abolished by concomitant atropine. This finding suggests that the relaxing effect of GLP-1 on the proximal stomach is mediated by inhibition of vagal cholinergic activity. Nevertheless, further studies are required to fully elucidate the mechanisms which mediate the gastric motor effects induced by GLP-1.
Fundus relaxation with GLP-1 is functionally relevant in that fundus pressure regulates gastric emptying of liquids.15 Reduced intragastric pressure is suggested to markedly contribute to the retardation of liquid emptying induced by this peptide. GLP-1 has been shown to decelerate liquid emptying both in human and pig models.7, 8, 40 Although the functional importance of phasic volume events has not been finally defined41 these pressure events are also considered to control liquid emptying.42 The present study suggests an enterogastrone effect of intestinally released GLP-1 in terms of fundus volume waves. Reduction of these pressure events may be another important mechanism whereby GLP-1 retards gastric emptying of liquids. Moreover, liquid emptying is accelerated in early stage type 2 diabetes without autonomic neuropathy.42 In line with rapid emptying of the fundus both scintigraphic and ultrasonographic studies revealed decreased accommodation of the proximal stomach in diabetics.17, 43 Thus apart from stimulating insulin and inhibiting glucagon release, gastric relaxation and inhibition of phasic volume events with subsequent reduction of intestinal glucose load may offer another mechanism for GLP-1 to improve glucose tolerance.
The interplay of fundus relaxation and dyspeptic symptoms currently attracts much attention. Enhancing fundus relaxation has been proposed as a novel approach to functional dyspepsia.16 In the present study, GLP-1 markedly relaxed the stomach at the operating pressure and each distension step. It increased gastric compliance but left gastric perception unaltered. Enhanced gastric volume is associated with an increase in wall tension during isobaric distension if wall tension is derived from Laplace's law. Wall tension has recently been suggested to be a controlling mechanism of perception.44 With GLP-1, the absence of an increase in perception would contrast with a raised wall tension (data not shown). This finding supports the concept that wall tension does not fully characterise the mechanics of the proximal stomach.20
During isobaric distension GLP-1 allowed the stomach to afford larger volumes before a certain degree of perception was reached. By relaxation of the stomach GLP-1 may alter the volume threshold at which stretch receptors are activated. The integrative effect of GLP-1 on motility and sensation of the proximal stomach is characterised by tolerance of greater intragastric volumes. In physiological and even pathophysiological states, the amount of intragastric volume tolerated is thought to be an appropriate measure reflecting the interplay of fundus tone and sensation. Uncomfortable perception of unphysiologically high intragastric pressures used in isobaric distension procedures may be less important. However, the 5-HT1 agonist sumatriptan relaxes the fundus and enhances food intake whereas GLP-1 relaxes the fundus and inhibits food intake.10, 11, 16 The α2 adrenergic agonist clonidine relaxes the fundus and reduces gastric sensation whereas the nitric oxide donor nitroglycerin relaxes the stomach without altering perception.20 These findings underscore that neither gastric sensation nor satiety are exclusively controlled by gastric mechanics. α2 Receptors along nociceptive pathways in the spinal cord, brainstem, and forebrain, and GLP-1 binding sites in circumventricular regions involved in the regulation of ingestion are examples of central mechanisms superimposing peripheral effects.20, 36
In conclusion, this study shows that GLP-1 relaxes the proximal stomach and reduces phasic volume events, arguably contributing to retarded emptying of liquids. This peptide is a candidate enterogastrone in terms of the fundus. Gastric relaxation may be beneficial in diabetic patients in that it slows intestinal nutrient exposure. GLP-1 allows the stomach to afford larger volumes without increase in sensation.
Acknowledgments
The authors are indebted to Michaela Junck, Gabriele Kraft, and Elisabeth Bothe for expert technical assistance. This study was supported by the Deutsche Forschungsgemeinschaft, grant No AR 149/1-2.