Article Text

Abstract
Objective Data on serial liver biochemistries of patients infected by different human coronaviruses (HCoVs) are lacking. The impact of liver injury on adverse clinical outcomes in coronavirus disease 2019 (COVID-19) patients remains unclear.
Design This was a retrospective cohort study using data from a territory-wide database in Hong Kong. COVID-19, severe acute respiratory syndrome (SARS) and other HCoV patients were identified by diagnosis codes and/or virological results. Alanine aminotransferase (ALT)/aspartate aminotransferase (AST) elevation was defined as ALT/AST ≥2 × upper limit of normal (ie, 80 U/L). The primary end point was a composite of intensive care unit (ICU) admission, use of invasive mechanical ventilation and/or death.
Results We identified 1040 COVID-19 patients (mean age 38 years, 54% men), 1670 SARS patients (mean age 44 years, 44% men) and 675 other HCoV patients (mean age 20 years, 57% men). ALT/AST elevation occurred in 50.3% SARS patients, 22.5% COVID-19 patients and 36.0% other HCoV patients. For COVID-19 patients, 53 (5.1%) were admitted to ICU, 22 (2.1%) received invasive mechanical ventilation and 4 (0.4%) died. ALT/AST elevation was independently associated with primary end point (adjusted OR (aOR) 7.92, 95% CI 4.14 to 15.14, p<0.001) after adjusted for albumin, diabetes and hypertension. Use of lopinavir–ritonavir ±ribavirin + interferon beta (aOR 1.94, 95% CI 1.20 to 3.13, p=0.006) and corticosteroids (aOR 3.92, 95% CI 2.14 to 7.16, p<0.001) was independently associated with ALT/AST elevation.
Conclusion ALT/AST elevation was common and independently associated with adverse clinical outcomes in COVID-19 patients. Use of lopinavir–ritonavir, with or without ribavirin, interferon beta and/or corticosteroids was independently associated with ALT/AST elevation.
- cholestasis
- hepatitis
- liver function test
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Significance of this study
What is already known on this subject?
Liver injury, in the form of hepatitis, cholestasis or both, can be observed in patients infected by different human coronaviruses (HCoVs).
ACE2, the host cell receptor in mediating entry of severe acute respiratory syndrome (SARS)-CoV and the recent SARS-CoV-2 has been demonstrated to express in cholangiocytes.
Liver injury is possibly caused by systemic inflammation and adverse drug reactions in severe coronavirus disease 2019 (COVID-19) patients who have been receiving different medical treatments.
What are the new findings?
The liver biochemistries of patients infected by different HCoVs changed dynamically during the infection, with abnormality observed at different time periods after infection.
The degree of liver injury could be impacted by coexisting chronic hepatitis in patients infected by HCoVs.
Alanine aminotransferase (ALT)/aspartate aminotransferase (AST) elevation and acute liver injury are independently associated with adverse clinical outcomes including admission to intensive care unit, use of invasive mechanical ventilation and/or death in COVID-19 patients after adjusted for presence of diabetes mellitus and hypertension, and albumin level.
Use of lopinavir–ritonavir, with or without ribavirin, interferon beta and/or corticosteroids was associated with ALT/AST elevation and acute liver injury in COVID-19 patients.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
Vigilant monitoring of liver biochemistries would be important regarding its dynamic change during infection and association with adverse clinical outcomes in COVID-19 patients.
Cautious use of appropriate medications with least hepatotoxicity would minimise liver injury in COVID-19 patients.
Thorough review of medical history and detailed investigation for concomitant liver diseases are crucial to improve patient outcomes.
Introduction
Coronaviruses (CoVs) are a large family of viruses that cause illness ranging from the common cold to severe pneumonia. CoVs are classified as a family within the Nidovirales order, viruses that replicate using a nested set of messenger RNAs.1 The human coronaviruses (HCoVs) are in two of these genera: alpha coronaviruses (HCoV-229E and HCoV-NL63) and beta coronaviruses (HCoV-HKU1, HCoV-OC43, severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East respiratory syndrome coronavirus (MERS-CoV) and the recently discovered SARS-CoV-2, previously called 2019 novel coronavirus (2019-nCoV)).2
Liver injury, either in the form of hepatitis, cholestasis or both, is commonly observed in up to 60% of patients suffering from SARS.3 Histological features include prominent mitoses, acidophilic bodies, Kupffer cells and mild to moderate lobular inflammation4; reverse transcriptase PCR (RT-PCR) positive for SARS-CoV was also found.5 As SARS patients often received antibiotics, antiviral medications, corticosteroids and even antifungals, part of the liver injury might have been contributed by the hepatotoxicity of some of these medications.5 In contrast, liver injury is not a common feature in MERS patients.6
The latest novel zoonotic coronavirus, SARS-CoV-2 first identified in late 2019 first in Wuhan, China, has resulted in more than 7.82 million confirmed cases and 430 000 deaths worldwide as of 15 June 2020.7 Raised alanine aminotransferase (ALT) and total bilirubin was reported in 28% and 18%, respectively, in one of the first reported coronavirus disease 2019 (COVID-19) cohorts,8 and up to 53% in subsequent series.9 Histologically, there was moderate microvascular steatosis and mild lobular and portal activity, indicating that the injury could have been caused by either SARS-CoV-2 infection or drug-induced liver injury.10 On the other hand, the impact of infections due to other HCoVs on liver is less well reported as those HCoVs usually cause mild upper respiratory tract symptoms, such that they would be managed at outpatient settings without close monitoring of liver biochemistries.
More importantly, whether liver injury is prognostically significant remains elusive. Due to the large number of patients infected by various HCoVs, in particular the fast growing number of COVID-19 patients worldwide, the impact of liver injury on clinical outcomes of COVID-19 patients and its predictors is important and the knowledge may affect the outcomes of many. Therefore, we aimed to compare the serial liver biochemistries of patients infected by various HCoVs, with special focus on the prognostic role of liver injury in COVID-19 patients, using a territory-wide cohort in Hong Kong.
Materials and methods
Study design and data source
We performed a territory-wide retrospective cohort study using data from the Clinical Data Analysis and Reporting System (CDARS) under the management of Hospital Authority, Hong Kong.11 CDARS is an electronic healthcare database that covers the patients’ demographic, death, diagnoses, procedures, drug prescription and dispensing history and laboratory results from all public hospitals and clinics in Hong Kong. It represents inpatient and outpatient data of around 80% of the 7.47 million population in Hong Kong.12 All confirmed SARS and COVID-19 patients were hospitalised in the public hospitals but not in private hospitals in Hong Kong. All data are deidentified in CDARS to ensure confidentiality. Different territory-wide studies of various infectious diseases were previously conducted using CDARS.13–15 The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding was used in CDARS. The use of ICD-9-CM codes in CDARS to identify medical conditions has been found 99% accurate when referenced to clinical, laboratory, imaging and endoscopy results from the electronic medical records.16
Subjects
Consecutive SARS patients from March to June 2003 were identified by ICD-9-CM diagnosis codes and/or virological results; consecutive laboratory-confirmed COVID-19 patients from 23 January 2020 to 1 May 2020 were identified by virological results and consecutive patients infected by other HCoVs from 1 January 2015 to 27 March 2020 were identified by virological results (online supplementary table 1). We reported the clinical characteristics of all identified patients. For subsequent analyses on serial liver biochemistries, we excluded patients who had missing ALT measurement at the time of diagnosis of HCoVs, and patients who had fewer than two ALT measurements during follow-up after the diagnosis of HCoVs. Patients were followed until death, last day of hospitalisation or last clinic visit, last follow-up date (24 May 2020) or up to 30 days of follow-up, whichever came first. Details on clinical evaluation and management of the patients were described in supplementary methods.
Supplemental material
Data collection
Data were retrieved from CDARS in 25 May 2020. Baseline date was defined as the date of diagnosis of COVID-19 or other HCoVs by virological results, or the date of ICD-9-CM diagnosis code of SARS and/or positive virological results of SARS. Demographic data including date of birth and sex were captured. Death and its date were captured and ascertained using data from CDARS and Hong Kong Death Registry. At baseline, haematological and virological parameters, liver and renal biochemistries, were collected. Thereafter, serial liver and renal biochemistries, as well as SARS-CoV or SARS-CoV-2 viral assays for patients infected by SARS-CoV or SARS-CoV-2 were collected until the last follow-up date (online supplementary table 1). We also retrieved data on other relevant diagnoses, procedures, concomitant drugs, laboratory parameters and exposure to antivirals, antibiotics and antifungals, corticosteroids, interferon beta and immunoglobulin during hospitalisation (online supplementary table 2).
Definitions of events
The primary end point was a composite end point of ICU admission, use of invasive mechanical ventilation and/or death. Use of invasive mechanical ventilation was defined by ICD-9-CM procedure codes (96.7). ALT/aspartate aminotransferase (AST) elevation was defined as ALT and/or AST≥2 × the upper limit of normal (ULN). Acute liver injury was defined as ALT and/or AST≥2 ×ULN, with total bilirubin ≥2 ×ULN and/or international normalised ratio ≥1.7. ULN of ALT and AST were defined according to the criteria of The Asian Pacific Association for the Study of the Liver (40 U/L for both genders).17 ULN of alkaline phosphatase (ALP) was defined by each of the local laboratory based on age and gender. ULN of total bilirubin was defined as 19 µmol/L. ULN of gamma-glutamyl transferase was 40 U/L.
Chronic hepatitis B and C were defined based on viral serology, use of antiviral treatment and/or ICD-9-CM diagnosis codes.14 Liver-related outcomes were defined based on ICD-9-CM diagnosis and procedure codes (online supplementary table 3). Significant comorbidities were defined as follows: hypertension was identified by use of any antihypertensive drug and/or ICD-9-CM diagnosis codes; diabetes mellitus (DM) was defined by exposure to any antidiabetic agent, haemoglobin A1c ≥6.5%, fasting plasma glucose ≥7 mmol/L in two measurements or ≥11.1 mmol/L in one measurement and/or the ICD-9-CM diagnosis codes for DM (250.00–250.93).18 Liver cirrhosis was identified by ICD-9-CM diagnosis codes for cirrhosis and its related complications (online supplementary table 3).
Statistical analysis
Data were analysed using Statistical Product and Service Solutions (SPSS) V.25.0 (SPSS) and R software (V.3.6.3; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed in mean±SD or median (IQR), as appropriate, while categorical variables were presented as number (percentage). Qualitative and quantitative differences between subgroups were analysed by χ2 test, χ2 test for linear trend or Fisher’s exact tests for categorical parameters and Student’s t-test or Mann-Whitney U test for continuous parameters, as appropriate. ORs and adjusted ORs (aORs) with 95% CI of ALT/AST elevation and acute liver injury on the primary end point were estimated by logistic regression. We adjusted for the following covariates: age, sex, presence of DM, hypertension, lymphopenia as defined by lymphocytes <1×109/L, platelet, albumin and creatinine; no patients were excluded in the analysis due to missing data. Backward stepwise selection was performed to select significant covariates. ORs and aORs with 95% CI of ALT/AST elevation and acute liver injury were estimated by logistic regression. We included the following covariates: use of lopinavir–ritonavir ±ribavirin, lopinavir–ritonavir ±ribavirin + interferon beta, corticosteroids, age, sex, presence of DM and hypertension; no patients were excluded in the analysis due to missing data. Hosmer-Lemeshow goodness-of-fit test was used to assess the goodness of fit of the model. All statistical tests were two-sided. Statistical significance was taken as p<0.05.
Results
Demographic characteristics
We first identified 1040 COVID-19 patients (all COVID-19 patients reported to the Department of Health) from 23 January 2020 to 1 May 2020, and 1670 SARS patients (95.2% of all SARS patients) from March to June 2003. We also identified 675 patients infected with other HCoVs (127 patients infected with HCoV-229E, 117 with HCoV-HKU1, 57 with HCoV-NL63 and 385 with HCoV-OC43 since January 2015) (figure 1); 4 patients had coinfection of HCoV-HKU1 and HCoV-OC43; 3 patients had coinfection of SARS-CoV-2 and HCoV-OC43; 2 patients had coinfection of HCoV-229E and HCoV-OC43; 2 patients had coinfection of HCoV-229E and HCoV-NL63; 1 patient had coinfection of SARS-CoV-2 and HCoV-229E and 1 patient had coinfection of HCoV-229E, HCoV-HKU1, HCoV-NL63 and HCoV-OC43.

Selection of patients infected with coronaviruses. ALT, alanine aminotransferase; HCoV, human coronavirus; SARS, severe acute respiratory syndrome.
At baseline, COVID-19 and SARS patients were older, had lower neutrophil, lymphocyte and platelet counts and had higher creatinine than patients infected by other HCoVs (table 1). At baseline, most of the patients had compensated liver function: serum albumin 40±6 g/L, total bilirubin 9±10 μmol/L, ALT (median (IQR)) 22 (15–35) U/L, 156/2282 (6.8%) and 8/1335 (0.6%) had chronic hepatitis B and C, respectively. Eight (0.2%) patients had liver cirrhosis: three were hepatitis B virus (HBV)-related, two were non-HBV-related and non-hepatitis C virus (HCV)-related, one was HBV-related and HCV-related, one was alcohol-related, while one had unknown aetiology (table 1).
Clinical characteristics of patients with various coronavirus infections
Liver test abnormality
Of note, 2434 patients were analysed on serial liver biochemistries (figure 1); all patients had serial measurements of ALT, total bilirubin and ALP. ALT/AST elevation occurred in 758 (50.3%), 184 (22.5%) and 40 (36.0%) of SARS patients, COVID-19 patients and patients infected in other HCoVs (table 2). The serum ALT levels peaked at median 12 (IQR 6–19) days in SARS patients, 8 (4–17) days in COVID-19 patients and 3 (0–11) in other HCoV patients. At day 30, 420/1202 (34.9%) SARS patients, 135/371 (36.4%) COVID-19 patients and 29/67 (43.3%) other HCoV patients had ALT normalised (online supplementary figure 1A-C). In COVID-19 patients, the median ALT level (IQR) was 22 (15–34) U/L at the time of first positive RT-PCR test and 23 (15–40) U/L at the time of first negative RT-PCR test (online supplementary figure 2A and B).
Abnormal liver biochemistries in the first 30 days after the diagnosis of coronavirus
Abnormal total bilirubin occurred in 954 (63.3%), 425 (52.1%) and 30 (27.0%) SARS patients, COVID-19 patients and patients infected in other HCoVs, respectively (table 2). The serum total bilirubin levels peaked at median 11 (IQR 8–16) days in SARS patients, 5 (3–9) days in COVID-19 patients and 2 (0–8) days in other HCoV patients. At day 30, 668/954 (70.0%) SARS patients, 351/425 (82.6%) COVID-19 patients and 20/30 (66.7%) other HCoV patients had total bilirubin normalised (online supplementary figure 3A-C). In COVID-19 patients, the mean total bilirubin was 8±5 μmol/L at the time of first positive RT-PCR test and 12±8 μmol/L at the time of first negative RT-PCR test (online supplementary figure 4A,B). Moreover, abnormal ALP occurred in 450 (29.9%), 69 (58.5%) and 44 (39.6%) SARS patients, COVID-19 patients and other HCoV patients, respectively (table 2 and online supplementary figure 5A-C). Acute liver injury occurred in 148 (9.8%), 15 (1.8%) and 11 (9.9%) of SARS patients, COVID-19 patients and patients infected in other HCoVs, respectively. Liver-related morbidity and mortality during HCoV infection were uncommon; two SARS patients had liver-related death (online supplementary table 4).
Patients with versus without chronic hepatitis
In COVID-19 patients, 31/760 (4.1%) and 2/609 (0.3%) had chronic hepatitis B and C, respectively. In SARS patients, 116/1363 (8.5%) and 4/599 (0.7%) had chronic hepatitis B and C, respectively. In patients of other HCoV infections, 9/163 (5.5 %) and 2/130 (1.5%) had chronic hepatitis B and C, respectively (table 1). Among 106 chronic hepatitis B patients who had available hepatitis B e-antigen status, 83.0% had negative hepatitis B e-antigen. Among 87 chronic hepatitis B patients who had available HBV DNA measurement, 56.3% had detectable HBV DNA with a median (IQR) of 849 (24–218 571) IU/mL, and 32 patients received HBV antiviral treatment. Patients with and without chronic hepatitis had a comparable proportion of ALT/AST elevation (48.5% vs 43.2%, χ2 test, p=0.186). The development of acute liver injury was significantly more in patients who had chronic hepatitis than those who did not have chronic hepatitis (15.0% vs 7.0%, χ2 test, p<0.001).
Abnormal liver biochemistries and clinical outcomes
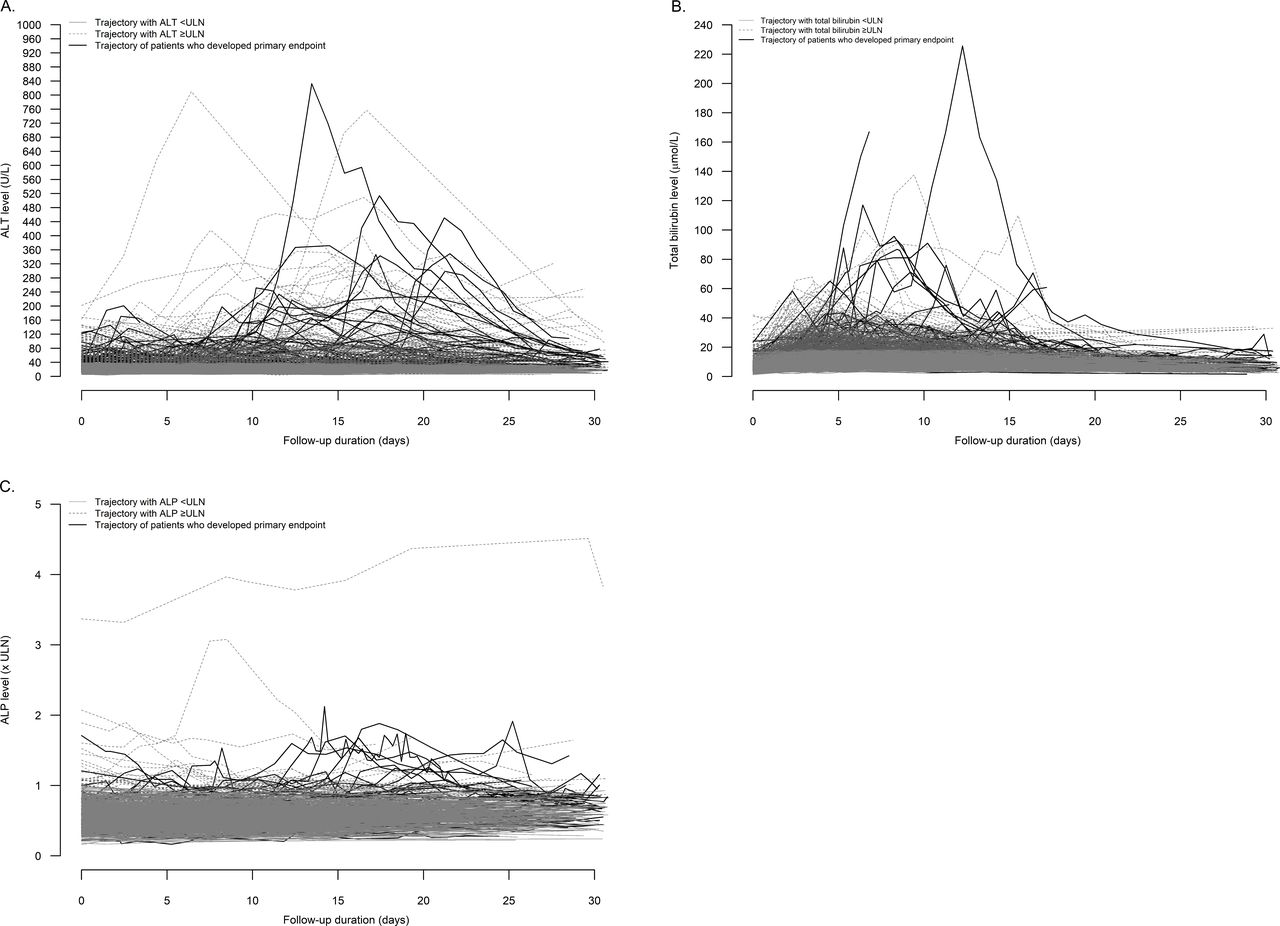
Of 1040 COVID-19 patients, 53 (5.1%) were admitted to ICU, 22 (2.1%) received invasive mechanical ventilation and 4 (0.4%) died. Of 1670 SARS patients, 336 (20.1%) were admitted to ICU, 61 (3.7%) received invasive mechanical ventilation and 286 (17.1%) died. Of 675 other HCoV patients, 49 (7.3%) were admitted to ICU, 40 (5.9%) received invasive mechanical ventilation and 19 (2.8%) died. Among 816 COVID-19 patients who had serial measurement of liver biochemistries, 184 (22.5%) had ALT/AST elevation and 15 (1.8%) had acute liver injury. More patients who developed primary end point, that is, a composite end point of admission to ICU, use of invasive mechanical ventilation and death, had abnormal liver biochemistries (table 3 and figure 2A-C). ALT/AST elevation and acute liver injury were more commonly seen in COVID-19 patients who developed primary end point than those who did not (ALT/AST elevation: 70.9% vs 19.1%, χ2 test, p<0.001; acute liver injury: 14.5% vs 0.9%, Fisher’s exact test, p<0.001).
Abnormal liver biochemistries during follow-up among patients infected by SARS-CoV-2 with or without primary end point (a composite end point of admission to intensive care unit, use of invasive mechanical ventilation and death)

{kind=link}
{kind=link}
(A) Serum ALT, (B) total bilirubin and (C) ALP of patients infected with SARS-CoV-2 who developed and did not develop primary end point. ALP, alkaline phosphatase; ALT, alanine aminotransferase; CoV, coronavirus; SARS, severe acute respiratory syndrome; ULN, upper limit of normal.
On univariate analysis, ALT/AST elevation, acute liver injury, older age, presence of DM, hypertension, low lymphocyte counts, platelet and albumin and high creatinine were associated with the development of primary end point (table 4). ALT/AST elevation was independently associated with the development of primary end point (aOR 7.92, 95% CI 4.14 to 15.14, p<0.001) after adjusted for significant confounding factors including presence of DM (aOR 4.14, 95% CI 1.96 to 8.71, p<0.001), hypertension (aOR 2.28, 95% CI 1.14 to 4.54, p=0.020) and albumin (aOR 0.92, 95% CI 0.87 to 0.98, p=0.005) on multivariable analysis (table 4). Similarly, acute liver injury was independently associated with the development of primary end point (aOR 6.40, 95% CI 1.78 to 23.07, p=0.005). For the 22 COVID-19 patients who received invasive mechanical ventilation, their mean age was 60±14 years; 12 (54.5%) were men; 15 (68.2%) and 14 (63.6%) had DM and hypertension, respectively. The peak ALT/AST and total bilirubin of the patients after the start of invasive mechanical ventilation were higher than the patients who did not use invasive mechanical ventilation (online supplementary table 5).
Univariate and multivariable analysis by logistic regression on factors associated with primary end point (a composite end point of admission to intensive care unit, use of invasive mechanical ventilation and death) in patients infected by SARS-CoV-2
Pharmacological treatment and abnormal liver biochemistries
Of 1040 COVID-19 patients, 377 (36.3%) patients have received antibiotics, 66 (6.3%) oseltamivir, 299 (28.7%) lopinavir–ritonavir ±ribavirin, 330 (31.7%) lopinavir–ritonavir ±ribavirin ± interferon beta and 59 (5.7%) corticosteroid therapy (5 methylprednisolone, 11 prednisolone and 51 hydrocortisone). Online supplementary figures 6A-7D show the serial ALT and total bilirubin of patients with reference to the start of lopinavir–ritonavir ±ribavirin and lopinavir–ritonavir ±ribavirin + interferon beta. We observed that ALT and total bilirubin were more likely to raise after the start of antiviral agents, while dropped gradually after the stop of antiviral agents. The serial ALP levels were relatively stable before and after the initiation and cessation of antiviral agents (online supplementary figure 8A-D).
ALT/AST elevation occurred in 30.2%, 19.2% and 15.0% of patients who used lopinavir–ritonavir ±ribavirin + interferon beta, lopinavir–ritonavir ±ribavirin, and those who did not used these antiviral agents (χ2 test for linear trend, p<0.001). On univariate analysis, ALT/AST elevation was more commonly seen in patients who received lopinavir–ritonavir ±ribavirin ± interferon beta, corticosteroids, had older age, male gender and presence of DM and hypertension (table 5). Use of lopinavir–ritonavir ±ribavirin + interferon beta (aOR 1.94, 95% CI 1.20 to 3.13, p=0.006) or corticosteroids (aOR 3.92, 95% CI 2.14 to 7.16, p<0.001) was independently associated with the development of ALT/AST elevation after adjusted for significant confounding factors including age and gender on multivariable analysis (table 5). Acute liver injury occurred in 2.8%, 2.1% and 0% of patients who used lopinavir–ritonavir ±ribavirin + interferon beta, lopinavir–ritonavir ±ribavirin, and those who did not used these antiviral agents (χ2 test for linear trend, p=0.027). Acute liver injury was more common in patients who used corticosteroids (aOR 4.76, 95% CI 1.56 to 14.50, p=0.006) than those who did not use (online supplementary table 6).
Univariate and multivariable analysis by logistic regression on factors associated with ALT and/or AST elevation in patients infected by SARS-CoV-2
Discussion
We report the serial liver biochemistries of COVID-19 patients, SARS patients and patients infected by other HCoVs. The liver biochemistries of patients infected by HCoVs changed dynamically during the clinical course. ALT/AST elevation and acute liver injury were observed in 23% and 2% of COVID-19 patients, respectively. Such biochemical changes have important implication, as ALT/AST elevation and acute liver injury were independently associated with admission to ICU, use of invasive mechanical ventilation and death.
So far, the exact impact of COVID-19 on the liver has not been well elucidated. A multicentre study in China reported the liver biochemistries of 32 COVID-19 patients (with four of them classified to have severe or critical type of COVID-19). All these four patients had abnormal ALT and total bilirubin that were 2–3 times higher than patients with mild-to-moderate COVID-19.19 Another study in China on 417 COVID-19 patients found that the prevalence of abnormal liver test and liver injury were high at admission and increased during hospitalisation. Use of lopinavir–ritonavir was associated with liver dysfunction. Patients with liver injury were more likely to develop severe COVID-19.20 Liver injury was believed to be caused by adverse drug reactions and systemic inflammation in severe COVID-19 patients who have been receiving medical treatment.10 19 Nonetheless, information on dynamic monitoring of liver biochemistries during hospitalisation, and clinical outcomes were less available in previous reports.19–21 Our study provided data on serial liver biochemistries of COVID-19 patients at admission and during hospitalisation and demonstrated that use of lopinavir–ritonavir ±ribavirin + interferon beta and corticosteroids was independently associated with ALT/AST elevation in COVID-19 patients. This association could be due to more severe disease in COVID-19 patients who received lopinavir–ritonavir ±ribavirin + interferon beta and corticosteroids. Use of corticosteroids was also associated with acute liver injury, while all 15 COVID-19 patients who developed acute liver injury also used lopinavir–ritonavir ±ribavirin ± interferon beta.
Our study showed that ALT/AST elevation and acute liver injury were independently associated with adverse clinical outcomes in COVID-19 patients. While our results were in concordance with previous publications that DM and older age were associated with adverse clinical outcomes,22 23 ALT/AST elevation as an independent factor could be a surrogate marker for inflammation due to COVID-19. While ALT/AST elevation and acute liver injury were independently associated with the need for ICU admission, mechanical ventilation and/or death in COVID-19 patients, no patients had liver-related mortality in short term. On the other hand, some patients who had elevated ALT, total bilirubin or ALP may have that normalised without the need of ICU admission or mechanical ventilation, as shown in figure 2. Regular monitoring of liver function in COVID-19 patients during hospitalisation would be important.
Different degrees of liver injury were observed in COVID-19 patients.9 24–26 The situation can also be complicated by coexisting chronic liver diseases. It would thus be essential to understand the natural course of liver injury in patients suffering from both COVID-19 and chronic liver diseases.27 We showed that acute liver injury was more commonly observed in patients infected by different HCoVs with chronic hepatitis. For COVID-19 patients, liver injury was reversible in short term in some of the patients, and no COVID-19 patients developed liver-related outcomes in short term. More prospective follow-up studies would be pivotal to understand the medium- to long-term liver-related outcomes of these patients.
SARS-CoV-2 is closely related to SARS-CoV.28 ACE2, the host cell receptor for SARS, has also been demonstrated in mediating COVID-19 infections.29–31 However, the exact reasons for the difference in adverse clinical outcomes between COVID-19 patients and SARS patients remain elusive. In our study, liver injury was more common among SARS patients than COVID-19 patients. SARS patients had more extensive use of antibiotics and antifungals, ribavirin and high-dose corticosteroid such as pulsed methylprednisolone. Hepatotoxicity of some of these medications may have contributed to part of the liver injury. The more advanced age and higher prevalence of DM and hypertension in SARS patients than COVID-19 patients may have also contributed to the difference in adverse clinical outcomes. On the other hand, the impact of infections due to other HCoVs on liver is less well studied as they are mostly managed in outpatient settings without serial monitoring on liver function. Although these HCoVs usually cause mild upper respiratory tract symptoms, we found that some patients could still develop abnormal liver biochemistries during infection, while short-term liver-related outcomes were rare. Yet, it is important to note that unlike SARS and COVID-19 patients who were all hospitalised, other HCoV patients who had serial liver biochemistries may represent the spectrum of patients with more severe disease. Patients who had mild disease and in a stable condition may not receive serial measurement of liver function. The proportion of HCoV patients with abnormal liver function is likely to be overestimated and needs to be carefully interpreted.
The strength of our study includes a territory-wide cohort that covers about 80% of the inpatient and outpatient services, and essentially all the SARS and COVID-19 cases in Hong Kong. Data from real-life cohorts represent a wider spectrum of patients such that the findings from real-life cohorts are thus more readily applicable to routine clinical practice. Nonetheless, our study has few limitations. First, we missed 85 out of 1755 (4.8%) of SARS patients in 2003 because of the diagnosis coding. Nonetheless, we believe missing about 5% of the SARS patients would not have major impact on the findings, as the proportion of deaths in our cohort (286/1670; 17.1%) was consistent with what was reported officially in 2003 (299/1755; 17.0%). Second, missing data of laboratory measurement might lead to biases as in other retrospective studies, though these biases can partially be compensated by our respectable cohort size. For SARS and COVID-19 patients, some less common laboratory parameters, such as C-reactive protein and erythrocyte sedimentation rate, might not be checked for every single patient due to minor variations of clinical practice in different hospitals. Yet, missing data were rare for common laboratory parameters including ALT, total bilirubin and ALP as those are regularly checked in our routine clinical practice. Missing data were more common among patients infected by other HCoVs as they are mostly managed in outpatient care settings. However, the amount of missing data of common laboratory parameters including ALT, total bilirubin and ALP were fewer. Third, ascertainment bias may affect the reliability of the study due to inaccurate entry of certain diagnosis codes for comorbidities, namely DM, hypertension and liver cirrhosis. We minimised this bias by including diagnosis, laboratory as well as medication data for DM and hypertension. We have also measured serum platelet counts and examined more definable ICD-9-CM codes for cirrhotic complications, which do not rely on a more accurate diagnosis of cirrhosis to identify the presence of cirrhosis.
In conclusion, liver injury was common and associated with adverse clinical outcomes in COVID-19 patients. Use of lopinavir–ritonavir ±ribavirin + interferon beta and corticosteroids was independently associated with ALT/AST elevation in COVID-19 patients. Vigilant monitoring of liver biochemistries and cautious use of appropriate medications with least hepatotoxicity would minimise such liver injury. In case of progressive liver injury, thorough review of medical history and detailed investigation for concomitant liver diseases are crucial to improve patient outcomes.
References
Footnotes
Contributors All authors were responsible for the study concept and design. GL-HW, TC-FY, YKT and GC-YL were responsible for the acquisition and analysis of data, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors were responsible for the interpretation of data, the drafting and critical revision of the manuscript for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TC-FY has served as an advisory committee member and a speaker for Gilead Sciences. GC-YL has served as an advisory committee member for Gilead, Merck and GSK, speaker for Merck and Gilead, and received research grant from Gilead, Merck and GSK. VW-SW has served as an advisory committee member for 3V-BIO, AbbVie, Allergan, Boehringer Ingelheim, Echosens, Gilead Sciences, Intercept, Janssen, Novartis, Novo Nordisk, Perspectum Diagnostics, Pfizer, TARGET-NASH and Terns; and a speaker for Bristol-Myers Squibb, Echosens, Gilead Sciences and Merck. He has also received a research grant from Gilead Sciences. HLYC is an advisor for AbbVie, Aptorum, Arbutus, Hepion, Intellia, Janssen, Gilead, GSK, GRAIL, Medimmune, Merck, Roche, Vaccitech, VenatoRx, Vir Biotechnology; and a speaker for Mylan, Gilead and Roche. DS-CH has served as an advisory committee member for Roche. GL-HW has served as an advisory committee member for Gilead Sciences, as a speaker for Abbott, Abbvie, Bristol-Myers Squibb, Echosens, Furui, Gilead Sciences, Janssen and Roche, and received research grant from Gilead Sciences.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. The data were obtained from a third party and would not be publicly available. Deidentified patient data were collected from the Clinical Data Analysis and Reporting System (CDARS) under the management of Hospital Authority, Hong Kong. All patients’ data were deidentified in CDARS to ensure confidentiality.