Article Text

Statistics from Altmetric.com
We read with interest the recently described affections of the GI system in coronavirus disease (COVID-19).1 2 In addition to the effects on the gut, mild abnormalities in liver aminotransferase levels have been observed.3 4 We here report a previously non-described severe liver failure in a patient with COVID-19.
A 65-year-old man was admitted to our emergency department with fever up to 40°C, dry cough and dyspnoea. The chest CT scan showed typical features of COVID-19, such as ground-glass opacities and peripheral consolidations. A throat swab confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Aminotransferase concentrations were slightly increased (alanine aminotransferase (ALT) 69 U/L and aspartate aminotransferase (AST) 92 U/L; upper limit of normal (ULN) ≤49 U/L). He had been receiving long-term treatment with hydrochlorothiazide and ramipril for arterial hypertension as sole medications and had no history of liver disease.
The patient was admitted to the isolation ward and was given supplementary oxygen. He received piperacillin/tazobactam and azithromycin according to hospital standards, as well as paracetamol (1 g, up to two times per day). Due to progressive respiratory failure and hyperventilation, mechanical ventilation was initiated on day 2.
In the further course ritonavir and lopinavir in combination with interferon beta were administrated from day 3 to days 10 and 13, respectively. This treatment was stopped due to progression of liver dysfunction and novel data showing lack of benefit.5
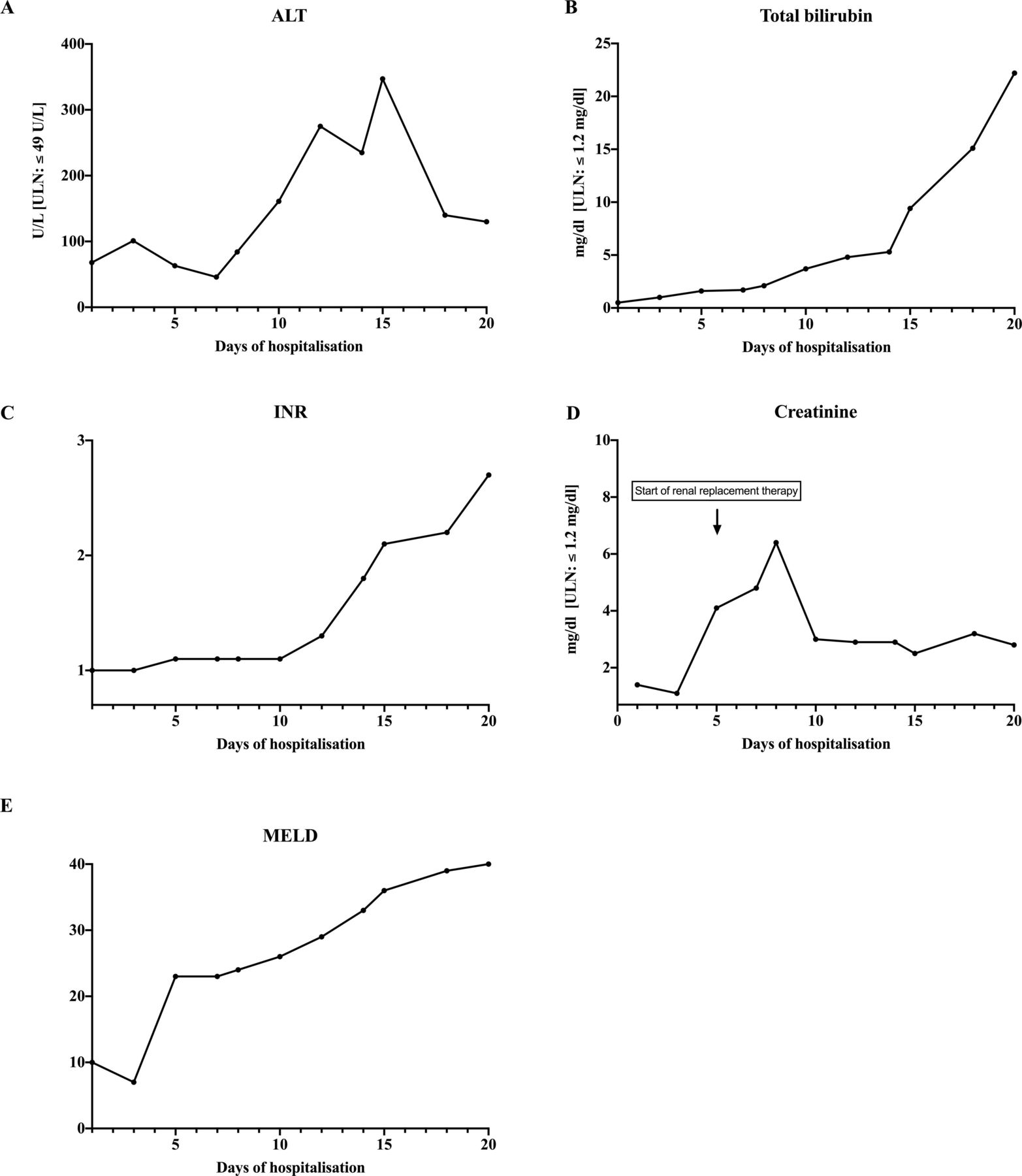
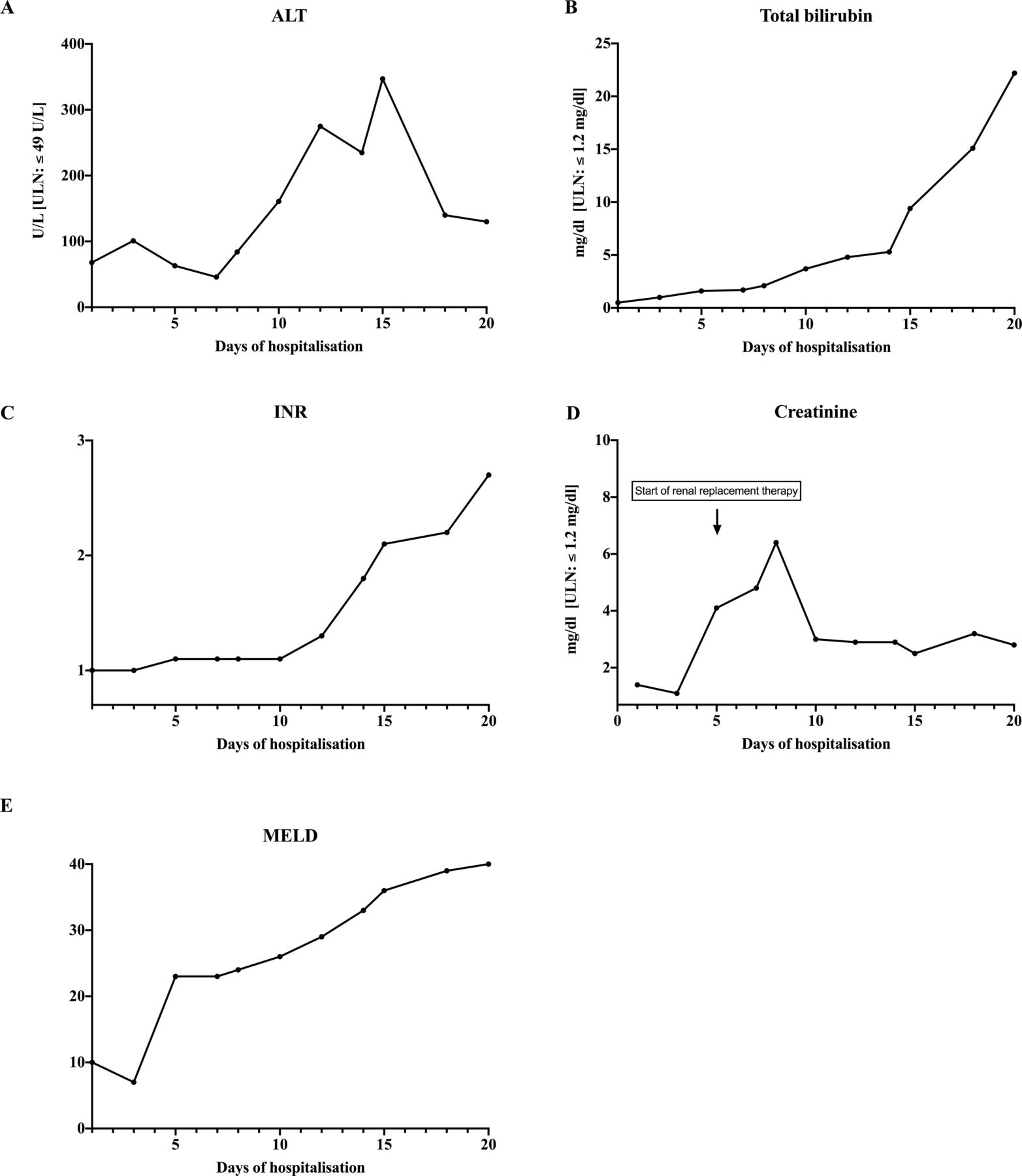
The patient developed mild to moderate acute respiratory distress syndrome with a minimal Horowitz index of 123 mm Hg and initially needed vasopressor therapy with a maximal dosage rate of 1.6 mg/hour (online supplementary figure 1). While oxygenation improved and vasopressor therapy could be reduced, serum aminotransferases started to increase on the seventh day and reached a maximum ALT of 465 U/L and AST of 746 U/L (ULN ≤49 U/L) on day 14 (figure 1A). Simultaneously, progressive elevation of total bilirubin to a maximum of 22.2 mg/dL (ULN ≤1.2 mg/dL) on day 20 was observed (figure 1B). With a delay of a few days, impairment of the coagulation was detected (figure 1C). Renal function also deteriorated and on day 5 continuous renal replacement therapy was initiated (figure 1D). Other causes of acute liver injury were excluded, such as viral hepatitis A, B, C and E and autoimmune hepatitis. Ultrasound of the liver did not show pathological findings, particularly no cholestasis nor hepatic perfusion disorders. Impairment of cardiac function was excluded by repeated echocardiography.
Supplemental material
{kind=link}
Evolution of alanine aminotransferase (ALT) (A), total bilirubin (B), international normalised ratio (INR) (C), creatinine (D) and Model for End-Stage Liver Disease (MELD) (E) until day 20 of hospitalisation. ULN, upper limit of normal.
At the time of the last follow-up (day 20), despite further therapeutic measures, the patient remained in a critical clinical situation with multiorgan failure, predominated by liver and kidney failure as illustrated by a score of 40 in the Model for End-Stage Liver Disease (figure 1E).
SARS-CoV-2 also uses the ACE2 receptor to enter target cells in the respiratory tract.6 Since an increased expression of ACE2 receptors has been described on cholangiocytes,7 a suspected mechanism of liver injury is the direct binding of SARS-CoV-2 to cholangiocytes. ACE inhibitors and angiotensin receptor blockers lead to enhanced ACE2 expression, raising the risk of a more severe outcome.8 Our patient had been treated with ramipril before SARS-CoV-2 infection, which may have increased the severity of liver damage. An additional cause of liver impairment in patients with COVID-19 might be drug hepatotoxicity. Our patient was given ritonavir and lopinavir, two antiviral drugs with known hepatotoxic potential.9 However, the diagnosis of drug-induced liver injury is by exclusion of other causes and therefore not feasible in our patient.10 Furthermore, secondary sclerosing cholangitis or hepatic vascular occlusion might have contributed to liver dysfunction in this patient. Yet no signs were observed by ultrasound. Moreover, cardiac function was preserved throughout and hypoxaemia was avoided due to early mechanical ventilation, lowering the risk for ischaemic hepatitis. Thus, additional causes, especially liver failure secondary to multiorgan failure, cannot be fully excluded in our patient. However, while elevated liver aminotransferase levels have been observed in SARS-CoV-2 infection, severe liver failure has not been described in similar circumstances as yet.1
Therefore, close monitoring of liver function seems warranted, and more research is needed to reveal the risk factors for liver failure in patients without pre-existing liver disease.
Footnotes
Contributors SW: data collection, first draft of the manuscript. JM, MI and ALG: supervision and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.