Article Text

Statistics from Altmetric.com
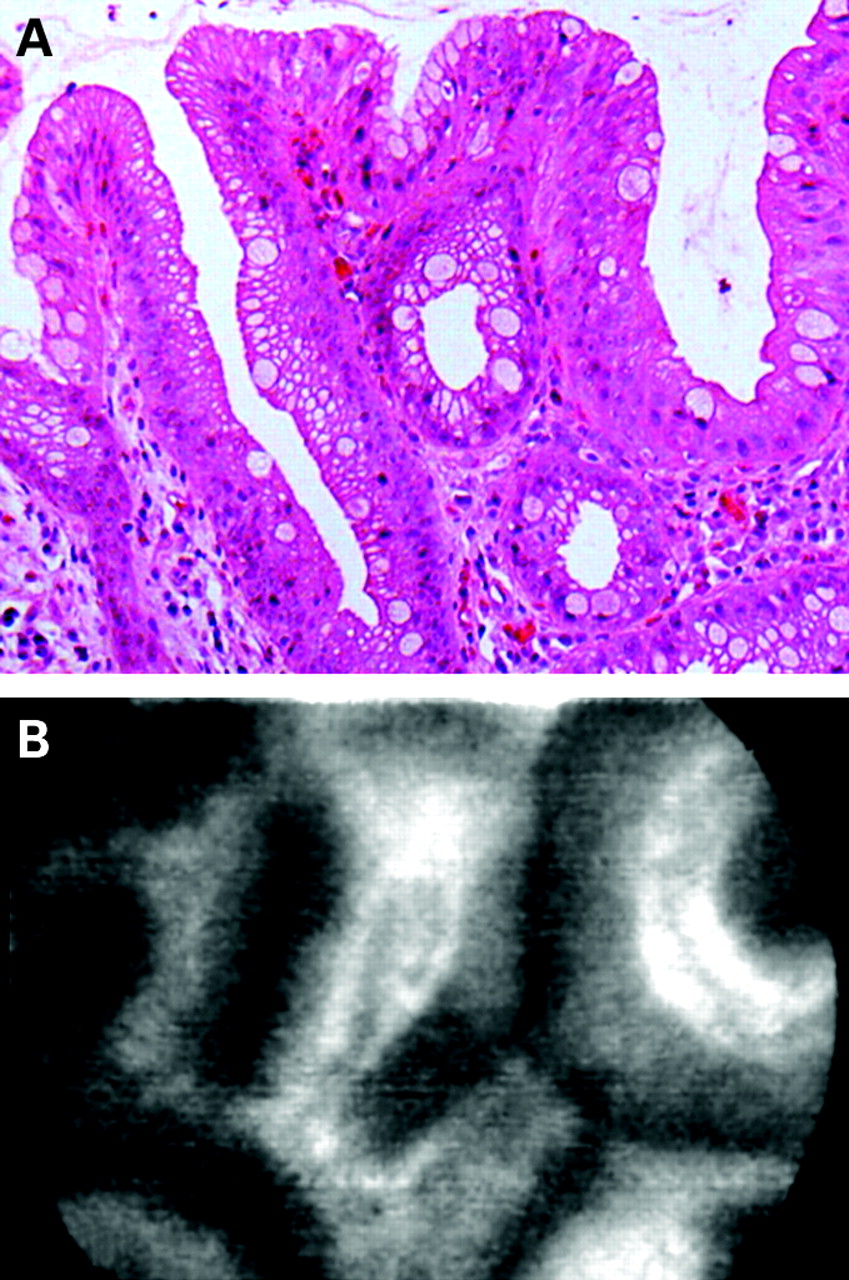
Miniprobe confocal laser microscopy demonstrates good negative but poor positive predictive value for invisible neoplasia in Barrett’s oesophagus
Better new techniques to highlight and characterise neoplastic changes in patients with Barrett’s oesophagus, beyond what can be seen with conventional high-resolution endoscopy techniques, are needed. Confocal laser microscopy (CLM) provides images at a cellular level and has shown promising results in the diagnosis of high-grade intraepithelial neoplasia or early carcinoma in patients with Barrett’s oesophagus. In this study, Pohl and colleagues evaluated a newly developed miniprobe CLM, which can be passed through the working channel of a standard endoscope, for the detection of invisible Barrett’s neoplasia. Initially, CLM imaging criteria for normal versus neoplastic Barrett’s oesophagus were developed. Thereafter, the accuracy values of these were tested, by matching CLM recordings to biopsy sites (see fig). The miniprobe CLM showed a high negative predictive value (99%) for the diagnosis of invisible Barrett’s neoplasia but the sensitivity needs to be improved (80%). This technique now needs to be evaluated in a larger cohort of patients with Barrett’s oesophagus, addressing the additional yield of CLM relative to standard high-resolution endoscopy with random four-quadrant biopsies only, which is the standard procedure at most sites today. See page 1648
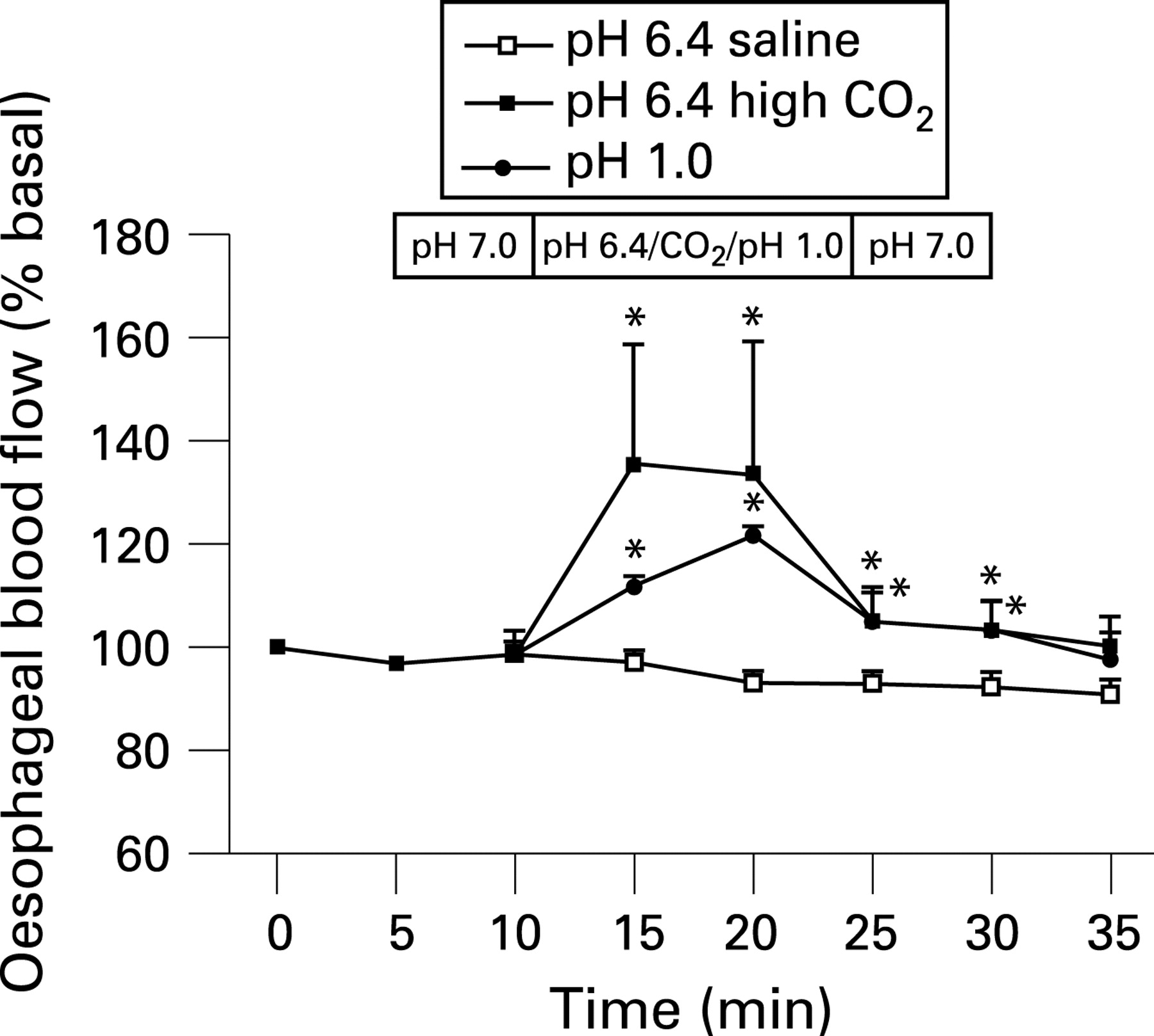
Is CO2, the permeant gas, responsible for the sensation of heartburn?
Heartburn and regurgitation, the key symptoms of gastroesophageal reflux disease, are related to the presence of oesophageal acid reflux. However, the amount of acid permeation across the mucosa in vivo in order to stimulate afferent nerves is negligible. In this issue of Gut, Akiba and co-authors provide evidence suggesting that CO2, not H+, is the permeant gas responsible for sensation of luminal acidity in the human oesophagus. Using blood flow as a surrogate marker of neural activation (see fig) the experiments performed support that CO2, generated from gastric HCl and bicarbonate (pancreas, duodenum, stomach or oesophageal glands), diffuses through the epithelium and interacts with carbonic anhydrase and the acid sensors transient receptor potential vanilloid 1 and acid-sensing ion channel, thereby resulting in the transduction of the acid signal. Moreover, capsaicin-sensitive sensory afferent nerves also seem to be involved in this process. These authors suggest that their findings may have relevance especially for patients with non-erosive reflux disease and this group of patients is in need of better treatment options. See page 1654

Flip—a theraputic target for inflammatory bowel disease?
Patients with Crohn’s disease (CD) demonstrate accumulation of T lymphocytes in the gut, which has been suggested to be partly due to defects in Fas-mediated apoptosis. This has been linked to upregulation of Fas-associated-death domain-like interleukin 1-converting enzyme-inhibitory protein (Flip), which is an inhibitor of Fas-mediated apoptosis. Caprioli and co-workers assessed the molecular mechanisms that control Flip in CD. They demonstrated that Flip was upregulated both at the RNA and protein level—ie, at both the transcriptional and post-translational level—in patients with CD (see fig). By treating CD3+ T lymphocytes from patients with CD with inhibitors of nuclear factor-κB and Janus kinase 2/signal transducer and activator of transcription, both these pathways were shown to be involved in the transcriptional control of Flip in CD. Moreover, in normal gut—but not in inflamed—Flip was rapidly degraded via the ubiquitin–proteasome pathway. Based on these findings, selective suppression of Flip in order to trigger apoptotic programmes and dampen inflammatory pathways seems to be an attractive therapeutic target for inflammatory bowel disease (IBD). See page 1674

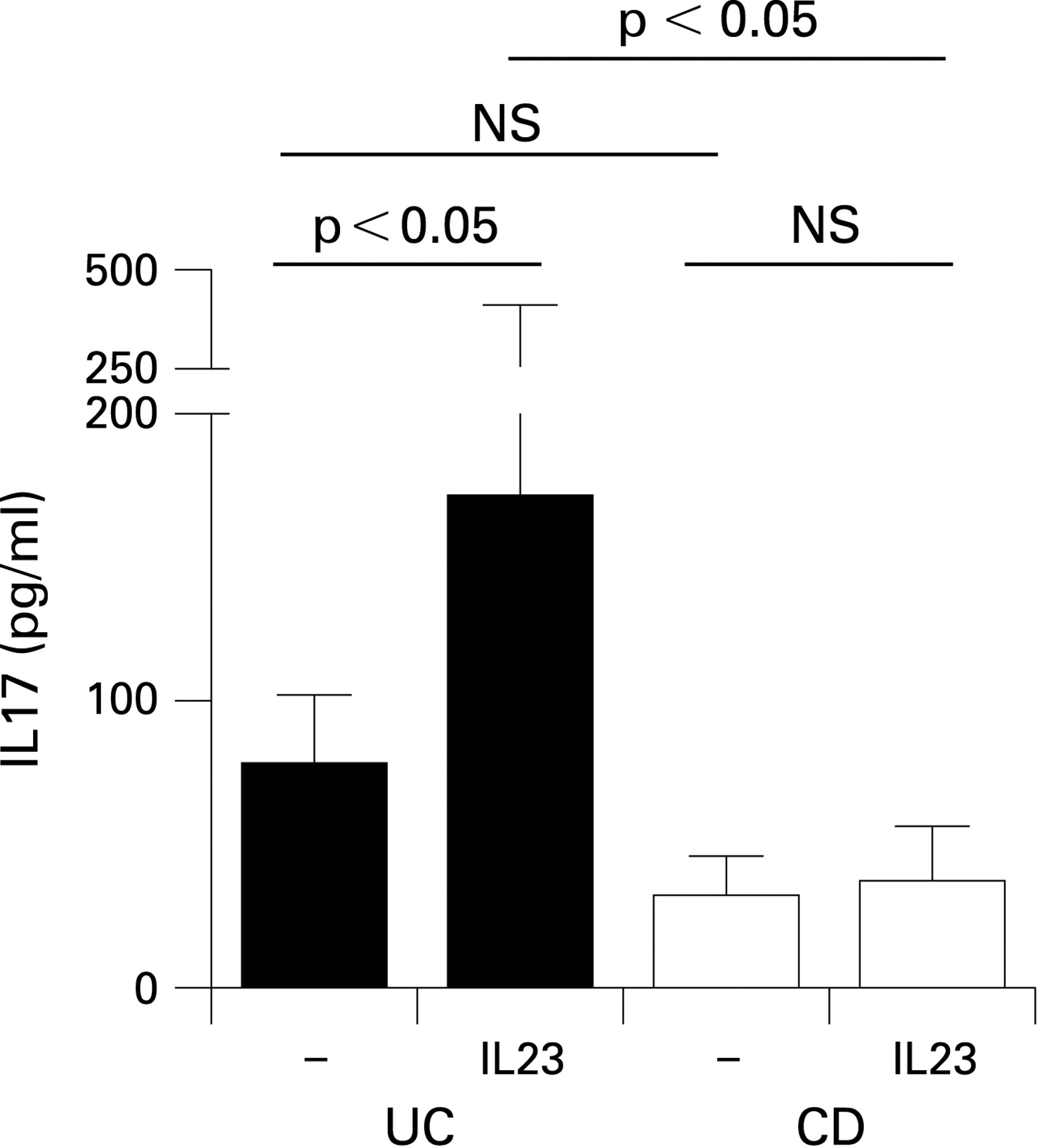
Th17/Th1 balance in ulcerative colitis and Crohn’s disease: key role of interleukin 23
The pattern of increased cytokines differs in ulcerative colitis (UC) and CD, something the study by Kobayashi and colleagues tries to explain. Seventy-five surgically resected specimens from 51 patients with UC and CD were examined for the production of cytokines in lamina propria CD4+ T cells. The most striking findings were an increase of interleukin (IL) 17 mRNA and IL17 production on stimulation in both conditions. Intracellular staining of T cells isolated from the lamina propria showed relatively more IL17 than interferon-γ in UC compared with CD. IL23 receptor was upregulated in both conditions but when cells were stimulated with IL23 only those with UC showed an increase in IL17 (see fig), while those with CD showed a greater increase in interferon-γ. The authors also showed that interferon-γ inhibited IL17 production and suggest that the differential effect of IL23 on CD4+ T cells accounts for the predominance of T helper (Th) 1 cytokines in CD as apposed to the Th17 predominance in UC. The authors conclude that the key role of IL23 suggests this may be an important future target for treating IBD. See page 1682

Value of a steroid trial in distinguishing autoimmune pancreatitis from pancreatic cancer
Autoimmune pancreatitis (AIP) causing obstructive jaundice may well masquerade as pancreatic cancer. A trial of steroids often produces a dramatic response but there have been concerns that using this to distinguish AIP from cancer may lead to cancer progression during the trial of steroids in an otherwise resectable patient. The rarity of AIP makes this series of 22 patients with clinically suspected AIP and atypical imaging of great value. Of the 22 patients, 15 showed a positive response to steroids (defined by a reduction of pancreatic mass and pancreatic duct obstruction at the follow-up CT scan performed at 2 weeks). Steroids were continued for 1 to 2 months followed by a gradual taper to a maintenance of 2.5–7.5 mg per day, which was continued for an average of 6 months. Although 20% of patients experienced a relapse of AIP, none developed malignancy. Seven of the patients did not respond to the 2-week steroid trial and all were shown to have pancreatic cancer either during surgery or during subsequent follow up. Although the numbers are small, the authors conclude that, even in patients in whom a pancreatic cancer might be an alternative diagnosis, a trial of steroids was safe and effective in making the final diagnosis of AIP and thus avoiding laparotomy. The authors are, however, keen to point out that the use of steroids to make a diagnosis should only follow thorough investigation in a centre of excellence to exclude malignancy including endosonography and fine-needle aspiration. See page 1704

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk factors for the development of acute and chronic hepatitis in China: impact of genotype
Despite a nationwide hepatitis B vaccination programme, mainland China has a third of the world’s hepatitis B virus (HBV) carriers. This study of the risk factors involved in infection and subsequent progression to chronic hepatitis in China is, therefore, of great significance. The authors performed a case–control study of 298 patients with acute hepatitis B who were matched with 624 controls. The strongest risk factor for acute hepatitis was lack of HBV vaccination, with an adjusted odds ratio (AOR) of 7.8, followed by invasive medical procedures (3.7), household contact with HBV carriers (3.1) and body care and beauty treatments in public places (1.5). Receiving a pedicure in a bath centre was a new factor detected in this survey, with an AOR of 1.98. Of the 294 patients, 25 progressed to chronic infection, an event which was more likely in older females and those infected with genotype C2 (see table). An AOR of 6.97 showed the genotype was an important independent predictor of risk. Defining the properties of C2 that lead to immune evasion is an important future goal. See page 1713
Linked Articles
- Oesophagus
- Oesophagus
- Intestinal inflammation
- Intestinal inflammation
- Pancreas
- Hepatology