Article Text

Statistics from Altmetric.com
TFF3 is a promising biomarker for screening for Barrett’s oesophagus
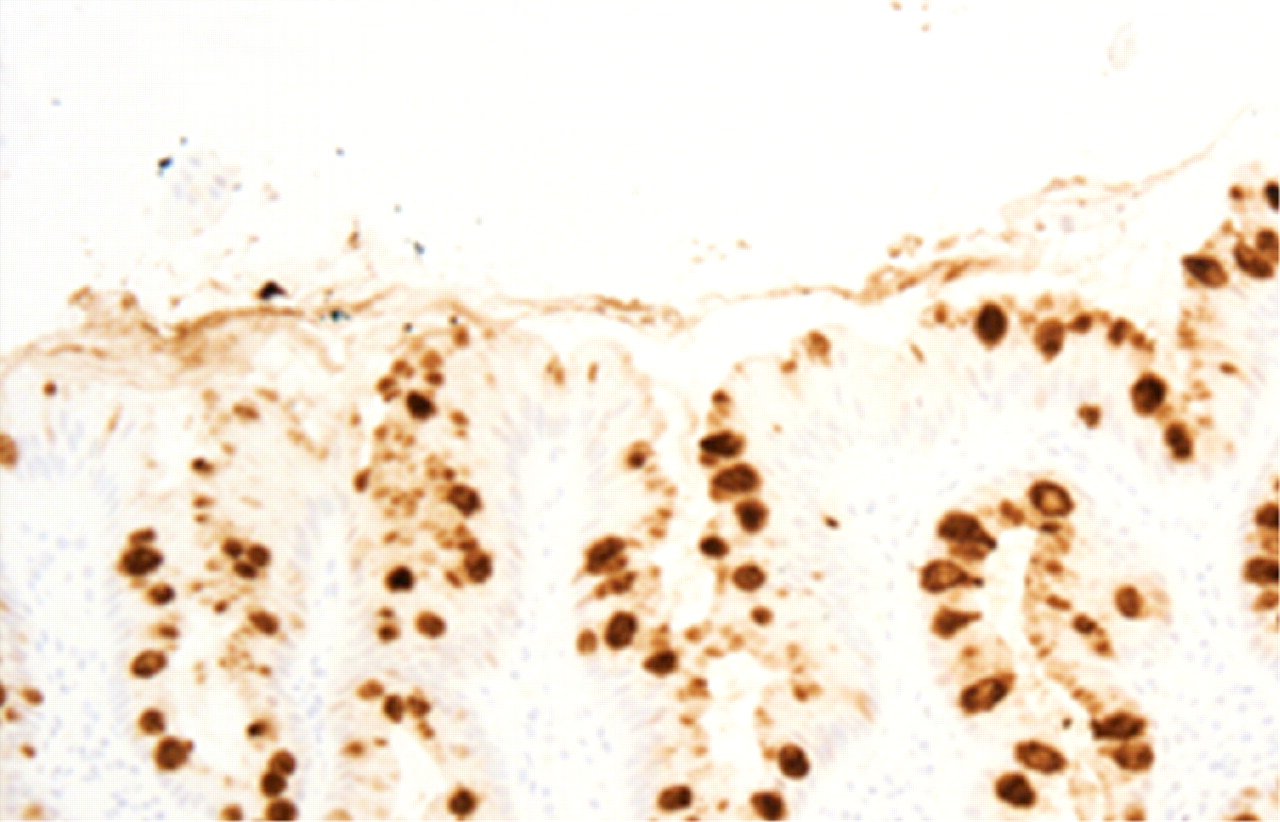
Economical ways of making an early diagnosis of Barrett’s oesophagus are essential if population screening is to be possible. The study by Lao-Sirieix and colleagues describes the use of a polyurethane sponge contained within a gelatine capsule attached to a string that is swallowed and retrieved after 3–5 minutes. Cells caught in the sponge are pelleted and processed immunohistochemically. Twenty-four candidate genes of possible biomarkers upregulated in Barrett’s oesophagus were identified from a review of published microarrays. Of these, dopa decarboxylase (DDC) and trefoil factor 3 (TFF3)were confirmed by real-time polymerase chain reaction to be over-expressed in oesophageal but not gastric biopsies from five patients with Barrett’s oesophagus and five healthy controls. Over-expression of TFF3 but not DDC was confirmed immunohistochemically in the oesophagus but not stomach of 21 patients with Barrett’s oesophagus and 20 controls (see fig). TFF3 was tested with the sponge capsule in 46 patients with >3 cm of Barrett’s oesophagus and 99 controls. Positive staining was seen in 36/46 patients and 6/99 controls, giving a sensitivity of 78%, specificity of 94% and a likelihood ratio of 13. This good performance could be enhanced in the future by DNA based assessment—such as methylation status or loss of heterozygosity—which could indicate the risk of progression to cancer.
See pages 1451
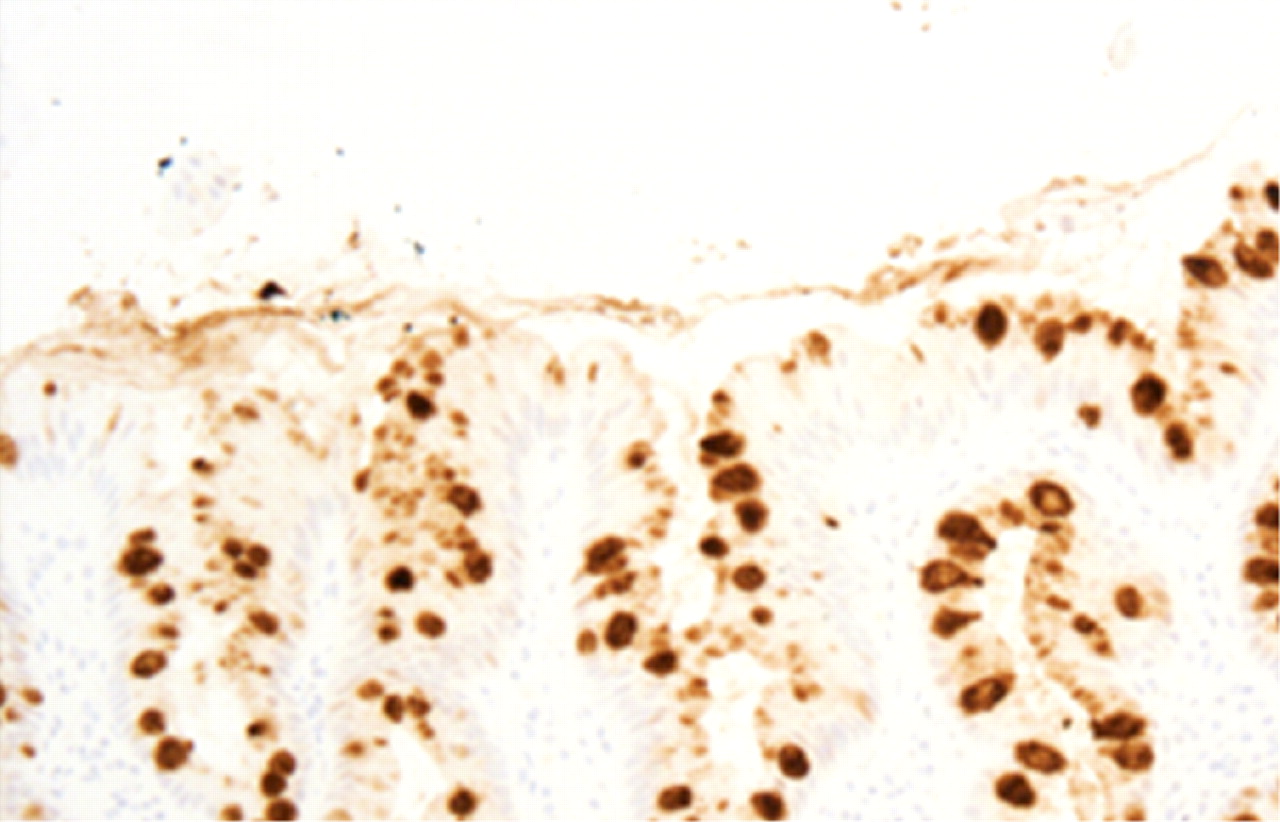
Barrett’s oesophagus strongly positive for trefoil factor 3 (TFF3) shown using immunohistochemical staining. The normal oesophagus showed no such stain.
Wireless capsule endoscopy is feasible and safe in young children
Wireless capsule endoscopy (WCE) has been widely used in adults but experience of its use in small children is limited. This European multicentre report describes 83 children <8 years old ( range 1.5–7.9 years) who were studied with WCE when routine endoscopy and radiology failed to explain their symptoms (see fig). Twenty children managed to swallow the standard Pillcam capsule (11 × 26 mm) but 63 required endoscopy. After initial experience with the Roth net revealed injuries to the oesophagus, the specifically designed Advance introducer was used exclusively. The commonest indication was obscure gastrointestinal bleeding (30) yielding a positive diagnosis in 16 ( ulcerative jejunitis 4, polyposis 4, angiodysplasia 2, blue rubber bleb 2 and Meckel’s diverticulum 2). Twenty were suspected Crohn’s disease with 11 positive diagnoses. The yield for other less common diagnoses including abdominal pain, protein losing enteropathy and malabsorption was around 50%. A major fear that has previously restricted use of WCE in children—namely capsule retention—was not observed. This study shows that capsule endoscopy is practical and safe, even in small children.
See pages 1467

Custom-made rucksack for batteries and recorder for small children.
Restraint stress increases permeability via CRF released from eosinophils
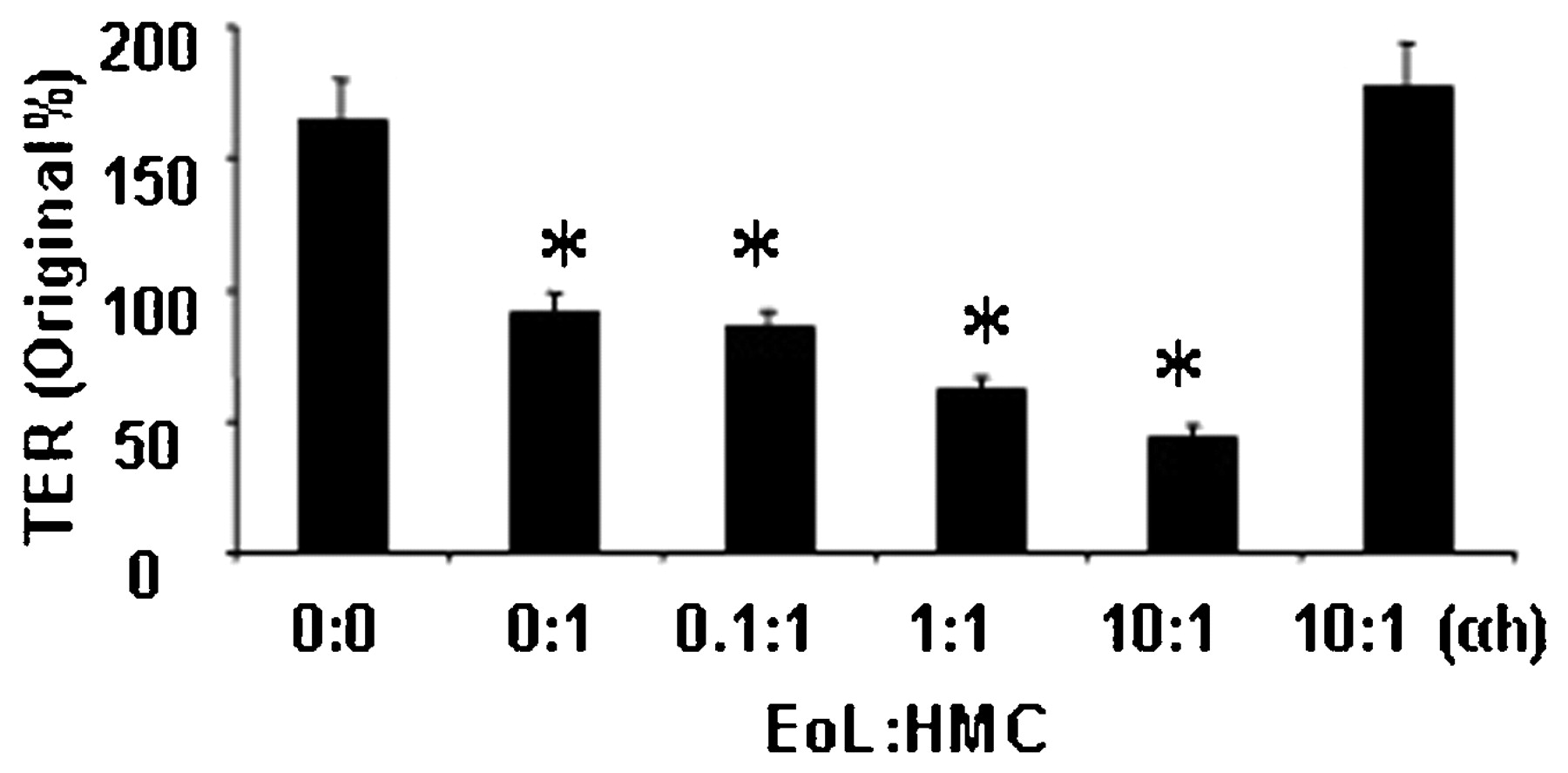
There is much current interest in the use of corticotrophin releasing factor (CRF) antagonists to treat stress-related gastrointestinal symptoms because animal studies suggest CRF is a major mediator. Stress increases gut permeability in animals, an effect that appears to be mediated by locally produced CRF since it can be blocked by peripherally acting CRF antagonists. The study by Zheng and co-authors found that stress induced the appearance of CRF in lamina propria immunocytes (mainly eosinophils). Various potential mediators were tested but only substance P (SP) was shown to induce CRF secretion by an eosinophil cell line. When exposed to SP and co-cultured with mast cells, these eosinophils increased the permeability of a cultured epithelial cell layer, an effect which could be blocked by CRF antagonist, α-helical corticotrophin releasing hormone (see fig). Further studies showed that SP did not alter epithelial barrier function directly but acted via CRF and required mast cells. This study shows for the first time one of the roles of eosinophils in the gut. Their activation by stress suggests that these might be targets for the treatment of stress-related disorders such as irritable bowel syndrome and functional dyspepsia.
See pages 1473

Effect on transepithelial resistance (TER) of co-culturing substance P (SP) primed eosinophil cell line (EoL) with human mast cells (HMC). Resistance fell with increasing numbers of eosinophils and could be restored by the corticotrophin releasing factor antagonist , α-helical corticotrophin releasing hormone.
Human intestinal epithelial cells promote the differentiation of tolerogenic dendritic cells
Immune homeostasis in the human gut is in part maintained by cross-talk between intestinal epithelial cells (IECs) and tissue resident dendritic cells (DCs). This is achieved via the induction of non-inflammatory DCs. In this study, the authors analysed whether IECs are involved in driving the development of tolerogenic DCs and whether dysregulations of this function occur in Crohn’s disease. From their experiments, they show that human IEC do indeed promote the differentiation of tolerogenic DCs able to drive the development of adaptive Foxp3+ Treg cells. This control is lost in patients with Crohn’s disease and paralleled a reduced expression of tolerogenic factors by primary IECs. Consistently, human primary CD103+ DCs isolated from mesenteric lymph nodes were endowed with the ability to drive Treg differentiation. This subset of DCs expressed CCR7 and probably represents a lamina propria-derived migratory population. In conclusion, the authors identified a population of tolerogenic CD103+ DCs in the human gut that are likely to differentiate in response to IEC-derived factors and drive the development of regulatory T-cells.
See pages 1481

Intestinal epithelial cells from patients with Crohn’s disease as opposed to controls show impaired ability to drive tolerogenic dendritic cells. (B) The graph represents pooled data from the experiments in (A).
Increasing incidence of paediatric inflammatory bowel disease in Ontario, Canada
Up to one-third of patients with inflammatory bowel disease (IBD) present under the age of 20. Data on trends in incidence and prevalence of childhood-onset IBD are conflicting. In this study from Ontario, Canada, a population-based clinical database of patients <15 years with IBD was studied and the patient information was linked to health administrative data to compare the accuracy of various patterns of healthcare use. The authors show that accurate identification of children with IBD required four physician contacts or two hospitalisations within 3 years if children underwent colonoscopy and seven contacts or three hospitalisations within 3 years in those without colonoscopy. The age- and sex-standardised prevalence of paediatric IBD increased from 42.1 in 1994 to 56.3 in 2005. The incidence per 100 000 increased from 9.5 in 1994 to 11.4 in 2005. Statistically significant increases in incidence were noted in 0–4 year olds (5.0% per year) and 5–9 year olds (7.6% per year), but not in 10–14 or 15–17 year olds. The authors conclude that there appears to be an accelerated increase in incidence in younger children.
See pages 1490
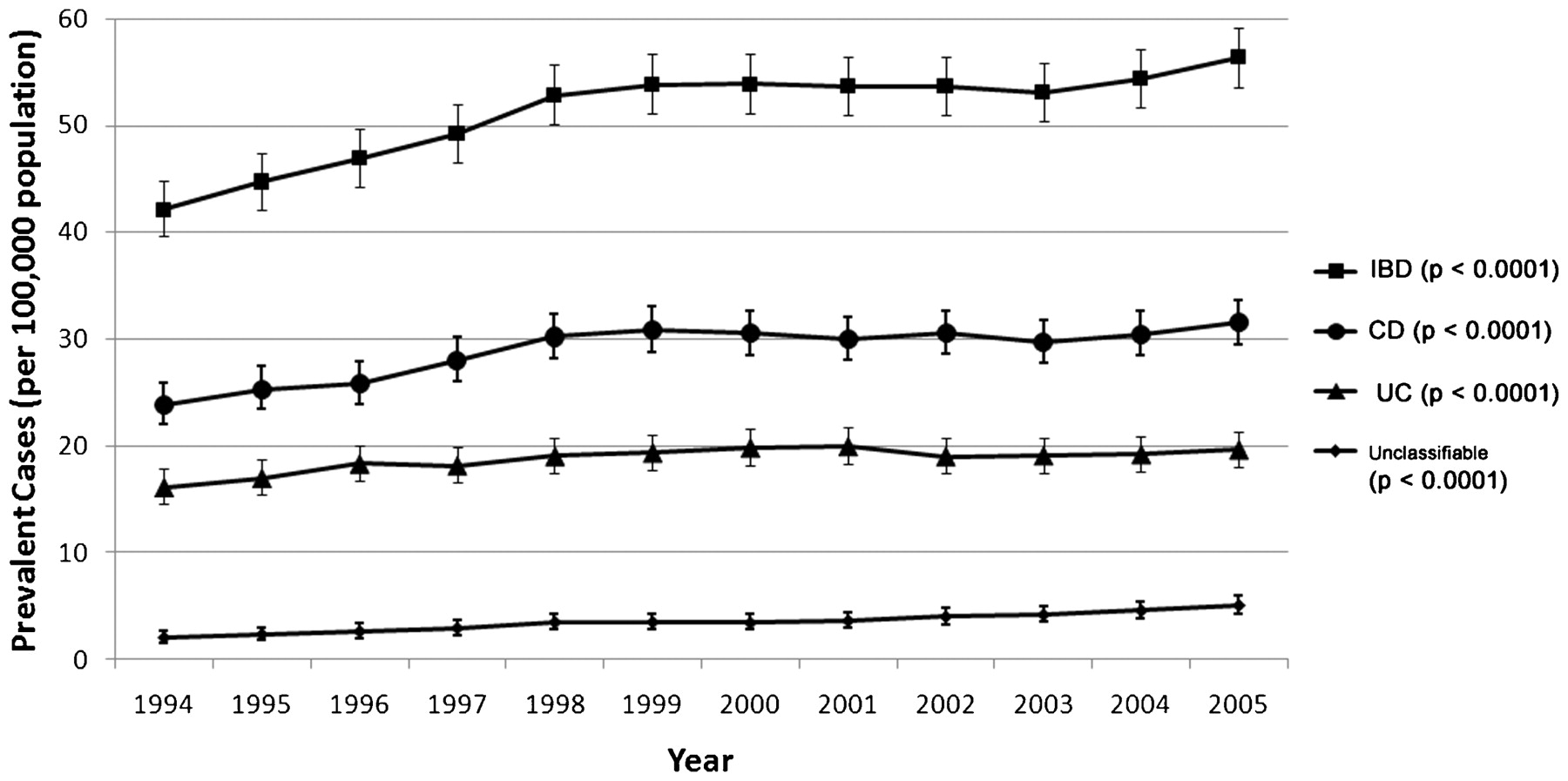
Age- and sex-standardised incidence of inflammatory bowel disease (IBD), Crohn’s disease (CD), ulcerative colitis (UC) and unclassifiable IBD per 100 000 population in Ontario, Canada.
Celecoxib induces hepatic stellate cell apoptosis through inhibition of Akt activation and suppresses hepatic fibrosis in rats
Activated hepatic stellate cells (HSCs)—but not quiescent HSCs—express cyclooxygenase-2 (COX-2), suggesting that the COX-2/prostanoids pathway plays a role in hepatic fibrogenesis. However, the role of COX-2 inhibitors in hepatic fibrogenesis remains controversial. In this animal study, the authors investigated the antifibrotic effects of celecoxib, a selective COX-2 inhibitor. Hepatic fibrosis was developed by bile duct ligation (BDL) or peritoneal thioacetamide (TAA) injection in rats. They demonstrate that celecoxib inhibited HSC proliferation and induced HSC apoptosis. All the COX inhibitors they studied completely inhibited prostaglandin E2 and prostaglandin I2 production in HSCs and attenuated extracellular signal-regulated kinase activation but only celecoxib significantly inhibited serine/threomine protein kinase B (Akt) activation in HSCs. Finally, oral administration of celecoxib (20 mg/kg/day) significantly decreased hepatic collagen deposition and α-smooth muscle actin expression in both BDL and TAA rats. They conclude that celecoxib shows pro-apoptotic effect on HSCs through Akt inactivation and anti-fibrogenic effects, suggesting celecoxib as a novel anti-fibrotic agent of hepatic fibrosis.
See pages 1517

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
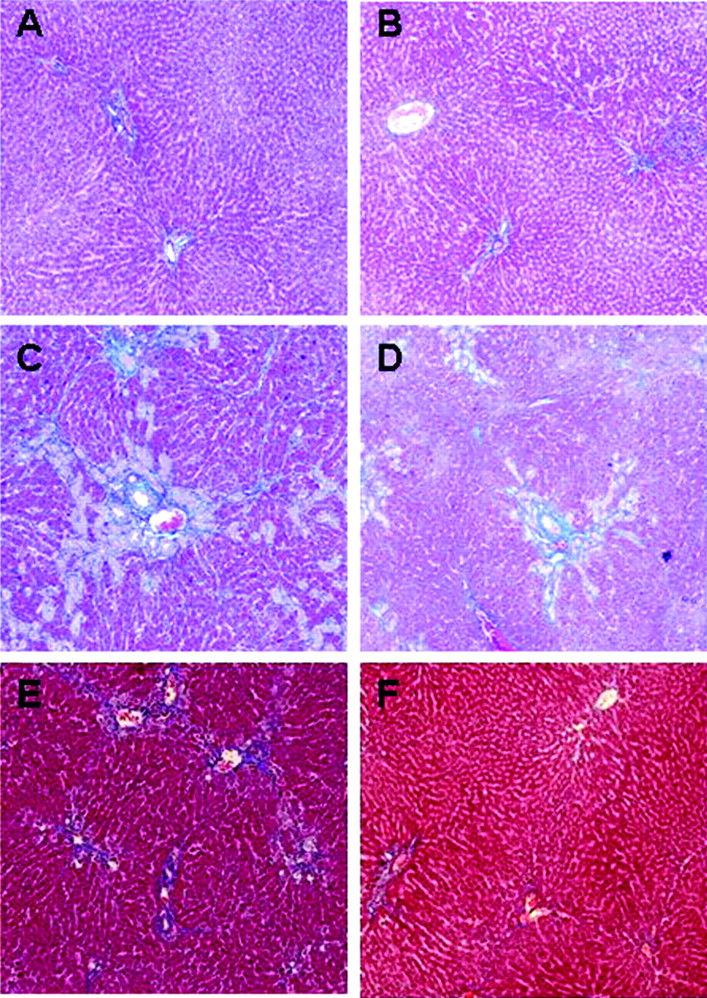
Anti-fibrotic effect of celecoxib in bile duct ligation- (BDL) and peritoneal thioacetamide- (TAA) induced hepatic fibrosis rat models. Histopathological findings of trichrome staining in livers of representative rats. Sham-operated rats were either treated with (A) placebo or (B) celecoxib (20 mg/kg/d) for 4 weeks. BDL-rats were either treated with (C) placebo or (D) celecoxib (20 mg/kg/d) for 4 weeks. TAA-rats were either treated with (E) placebo or (F) celecoxib (20 mg/kg/d) for 5 weeks.
Linked Articles
- Hepatology
- Oesophagus
- Neurogastroenterology
- Inflammation
- Small intestine
- Inflammatory bowel disease