Article Text

Statistics from Altmetric.com
Association of adiponectin with Barrett’s oesophagus
Obesity is a known risk factor for both Barrett’s oesophagus and reflux. The current study explores the possibility that the link with obesity is due to metabolic factors rather than reflux alone. Adiponectin is secreted by adipose tissue into the blood in multimeric complexes, trimers (low molecular weight, LMW), hexamers (middle molecular weight, MMW) and octadectimers (high molecular weight HMW) and total blood levels are inversely related to obesity. While HMW are pro-inflammatory, LMW are anti-inflammatory. This study examined 311 subjects undergoing endoscopy for reflux symptoms or Barrett’s surveillance. They found the ratio of LMW/Total adiponectin to be decreased in Barrett’s oesophagus particularly in females (figure). High LMW was associated with reduced risk of Barrett’s versus low LMW, OR 0.33 while the top tercile of the LMW/total ratio compared with the lowest tercile had an OR of 0.27 (0.13 – 0.58) overall and 0.2 for women alone. The authors conclude that it is the balance of the anti- and pro-inflammatory forms of Adiponectin that determine whether reflux leads to Barrett’s oesophagus. See page 1582

Box plot showing ratio of LMW/total Adiponectin stratified by gender in cases of Barrett’s and controls with just reflux.
NSAID induced small intestinal ulceration is increased by insoluble dietary fibre
Small intestinal (SI) ulceration due to NSAIDs is of increasing clinical importance. Non-specific cyclooxygenase inhibitors such as indomethacin (IND) induce a compensatory increase in leukotriene synthesis associated with ileal hypermotility. The current study examined the impact of insoluble dietary fibre on IND-induced SI injury which was strikingly increased on a high fibre diet (HFD) particularly in the distal SI. IND-induced ileal hypermotility was likely due to leukotriene since it was inhibited by AA-861 a 5-lipoxygenase inhibitor and pranlukast (a LT receptor antagonist) and atropine (see figure). These intestinal lesions were also inhibited by treatment with cholestyramine and neomycin suggesting that bile salts and luminal bacteria also play a role. IND may stimulate ileal motility by inhibiting the production of inhibitory prostaglandins (PGI2 & PGE2) and increasing the production of stimulatory leukotrienes. This regional hypermotility together with increased concentration of bile salts, insoluble fibre and bacteria may localise mucosal injury to the ileum. It remains to be seen whether differences in dietary fibre intake contribute to different susceptibilities to NSAID induced small intestinal injury in patients. See page 1590

Effect of AA-861, pranlukast and atropine on ileal motility induced by Indomethacin. All three significantly inhibited Indomethacin induced injury.
Linoleic acid and ulcerative colitis – a European prospective cohort study
Ulcerative colitis is a chronic inflammatory disease with a multifactorial etiology, including environmental factors. Dietary linoleic acid, an n-6 polyunsaturated fatty acid, is metabolised to arachidonic acid, which in turn is further metabolised to eicosonoids including prostaglandin E2, leukotriene B4 and thromboxane A2. These eicosanoids have pro-inflammatory properties and are found with excess in the mucosa of patients with ulcerative colitis. In this study, the authors investigated therefore if a high dietary intake of linoleic acid would increase the risk of ulcerative colitis. Over 200 000 individuals participating in the EPIC trial (European Prospective Investigation into Cancer and Nutrition) were followed up prospectively for the diagnosis of UC. Dietary data from food questionnaires were available and each case was matched with four controls. A total of 126 participants developed ulcerative colitis after a median follow-up of 4 years. The highest quartile of intake of linoleic acid was associated with an increased risk of ulcerative colitis (OR = 2.49, 95% CI 1.23 to 5.07, p = 0.01). The authors conclude that dietary linoleic acid may play a role in the aetiology of ulcerative colitis. See page 1606
Identification of major zymogen granule membrane glycoprotein GP2 as the autoantigen of pancreatic antibodies in Crohn’s disease
Crohn’s disease is associated with a number of (auto)antibodies, including pancreatic antibodies (PAB). The exact antigen to which PAB are directed is unknown. In the present study, the authors used immunoblotting and MALDI-TOF mass spectrometry, in order to identify the major antigenic target of PAB. The specificity of autoantibody reactivity was then confirmed by ELISA and indirect immunofluorescence (IIF) using purified rat and human recombinant GP2. The results of the immunoblotting and mass spectrometry analyses identified the major zymogen granule membrane glycoprotein 2 (GP2) as the autoantigen of PAB in CD. Immunohistochemistry confirmed GP2 expression in human colon biopsies from CD patients. Interestingly, the rat GP2 amino acid sequence exhibits 85% similarity to human Tamm-Horsfall protein and defective THP synthesis has been shown to increase the susceptibility of mice to urinary tract infections. It is tempting to speculate that GP2 secreted by the pancreas and not digested by zymogens could block the interaction of adhesive bacteria in the intestinal tract like THP does in the urinary tract. The authors conclude that quantification of anti-GP2 antibodies could improve the serological diagnosis of IBD. See page 1620

Median OD of anti-GP2 IgG antibodies determined by ELISA using purified rat GP2 in (A) PAB-positive CD patients (n = 42), (B) PAB-negative CD patients (n = 31), (C) UC patients (n = 49), and (D) Blood donors (n = 69)
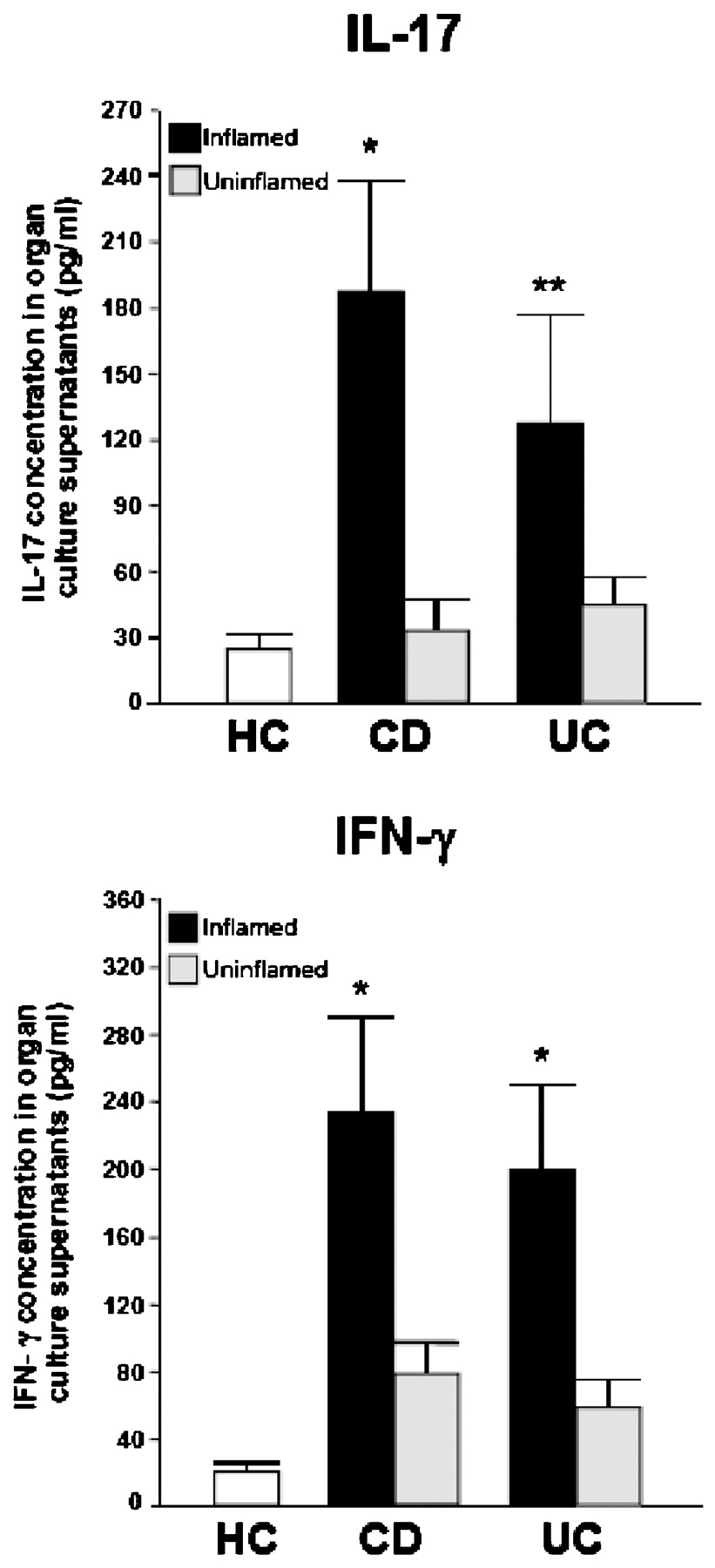
Differential regulation of interleukin-17 and interferon-gamma production in inflammatory bowel disease
IL-17 plays a role in a number of chronic inflammatory disorders but the mechanisms regulating its production in IBD are unclear. In the study by Rovedatti, endoscopic biopsies or surgical specimens were taken from inflamed and uninflamed colonic mucosa of IBD patients and normal colon of controls. IL-17 and IFN gamma were measured in the supernatants, and anti-CD3/CD28-stimulated LPMCs incubated with IL-12, IL-23, IL-1β plus IL-6, TGF-β1, or anti-IL-21 neutralising antibody. The authors show that IL-17 production was higher in IBD inflamed mucosa than uninflamed mucosa and controls, and was equivalent in amount to IFN-γ. Anti-CD3/CD28-stimulated IBD LPMCs produced more IL-17 than controls. IL-12 markedly increased IFN-γ production and decreased IL-17 production. TGF-β1 dose dependently decreased IFN-γ, but had no effect on IL-17 production. Blocking IL-21 significantly down-regulated IL-17 production. Taken together, the results support a role for IL-12, TGF-beta and IL-21 in modulating the IL-17/IFN-γ production in IBD. The increase in IL-17 in inflamed IBD mucosa may also help to explain why anti-IFN-antibodies failed to show efficacy in clinical trials of CD. See page 1629

Levels of IL-17 and IFN-γ in the supernatants of biopsies taken from the inflamed and uninflamed colon of 7 Crohn’s disease (CD) patients and 10 ulcerative colitis (UC) patients, and from the normal colon of 10 healthy controls (HC).
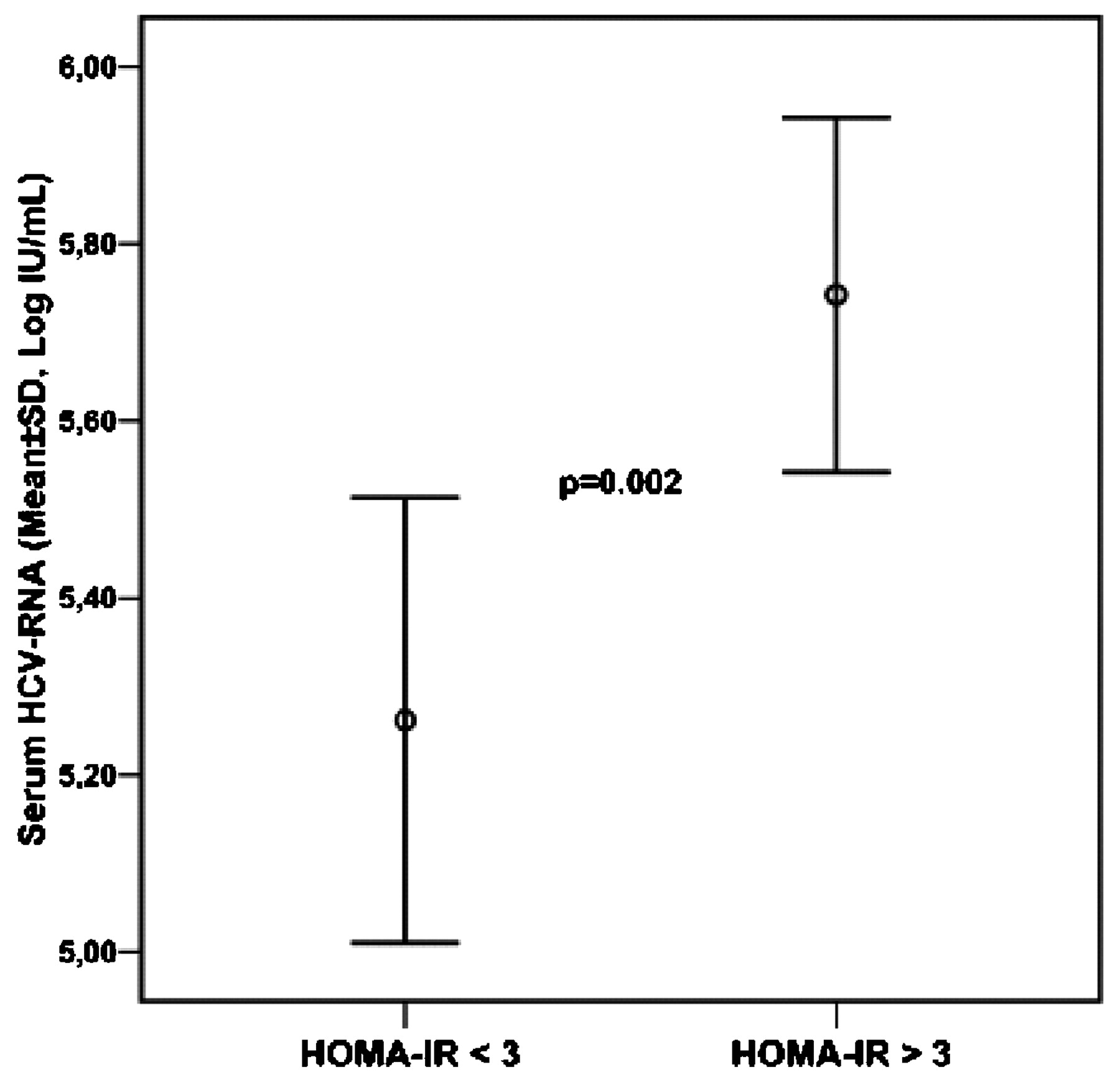
Association of insulin resistance with viral load in hepatitis C virus genotype 4 (HCV-4) infection
HCV-4 is the commonest type of HCV in the Middle East and Africa and is becoming increasingly important in Europe owning to migration and viral spread. Response to peginterferon and ribavirin is known to be influenced by both viral subtype and host factors which include fibrosis and insulin resistance. The current study performed in France examined the relative importance of these host factors in 266 patients with HCV-4 infection undergoing liver biopsy of whom 108 entered a trial of 48 weeks treatment with peginterferon ± ribavirin. Insulin resistance HOMA-IR >3 was associated with markedly higher levels of serum HCV RNA levels (figure). A multivariate analysis showed that the strongest predictor of sustained viralogical response (SVR) was Egyptian origin (Odds Ratio (OR) 13.1 (3.0–55.7) closely followed by the absence of severe fibrosis (METAVIR score F0-F2), OR 8.1 (2.5–25.9) and absence of insulin resistance HOMA-IR ( homeostasis model assessment of insulin resistance) <2, OR 5.3 (2.0–14.5). The strong relationship between insulin resistance and HCV- RNA levels raises the possibility of a direct role of virus in the development of insulin resistance. See page 1662
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Legend: Serum HCV-RNA level (mean with the SD) in patients with insulin resistance (HOMA-IR. >3) compared to those without insulin resistance (HOMA-IR <3).
Linked Articles
- Commentary
- Inflammatory bowel disease
- Small intestine
- Hepatology
- Inflammatory bowel disease
- Inflammatory bowel disease